





Abstract
The aim of this article is to present a rhinolithiasis patient with a significant asymmetric adenoid hypertrophy on the same side and to describe possible mechanisms for this clinical entity. Careful nasopharyngoscopy after removal of rhinolith is mandatory not to overlook significant adenoid hypertrophy which may interfere with patients’ symptoms. The role of paranasal CT scan in the diagnosis of an asymmetric adenoid hypertrophy in rhinolithiasis patients is also discussed.
INTRODUCTION
Adenoid hypertrophy (AH) is described as the non-physiological enlargement of the nasopharyngeal tonsils which may lead to nasal obstruction. There are several previously suggested histopathological mechanisms for adult AH, among them chronic nasal inflammation is the most popular one (1).
Rhinoliths develop within the nasal cavity as a result of mineralization of an endogenous or exogenous nidus. Rhinoliths cause rhinitis which may lead to complications including nasal polyps, atrophic rhinitis, septal perforation and oroantral fistula (2).
The aim of this article is to present a case with rhinolithiasis which also has ipsilateral asymmetric adenoid hypertrophy. Additionally, previous reports were reviewed for the presence of this clinical entity and possible mechanisms were described.
CASE REPORT
A 24 year old male presented with unilateral nasal obstruction. Additionally, the patient described ipsilateral facial pain and persistent purulent rhinorrhea. Nasal endoscopic examination revealed purulent secretion and a left sided mass which totally obstructed the nasal cavity. The mass had irregular contours, recovered by granulation tissue and was very hard and immovable on palpation with forceps. Nasal endoscopy was impossible on the left side and was normal on the right side with minimal nasopharyngeal adenoid hypertrophy.
A computed tomography (CT) was performed and a left sided mass in the inferior meatus which has demonstrated central calcification was reported (Figure 1). Mild mucosal hypertrophy was present in the left ethmoid and maxillary sinuses, accompanied with ipsilateral asymmetric adenoid hypertrophy (Figure 2).
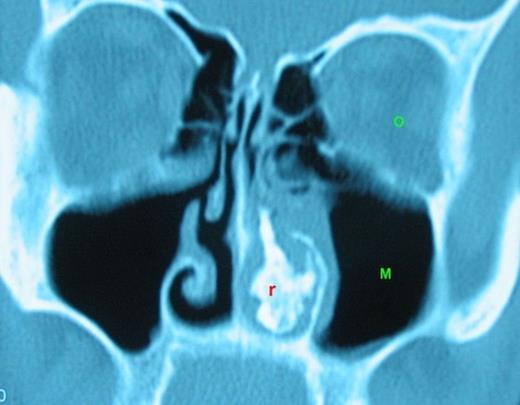
Rinolith is seen on the left nasal cavity. (r: rinolith, O: orbit, M: Maxillary sinus)
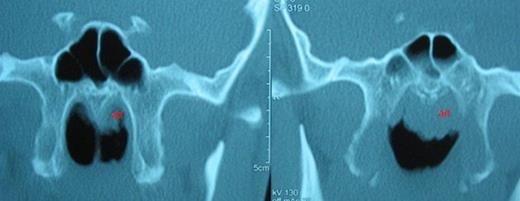
Asymmetric adenoid hypertrophy, more prominent on the left side. ad: adenoid hypertrophy
The patient underwent endonasal endoscopic surgery with the diagnosis of rhinolithiasis. The rhinolith was successfully removed with minimal possible injury to surrounding nasal mucosa. The nasal cavity was irrigated with saline. After removal of the rhinolith, adenoid hypertrophy was prominent on the left side (Figure 3). Adenoidectomy was subsequently performed and postoperative histopathologic examination revealed lymphoid hyperplasia and chronic inflammatory cell infiltration without any malignant transformation.
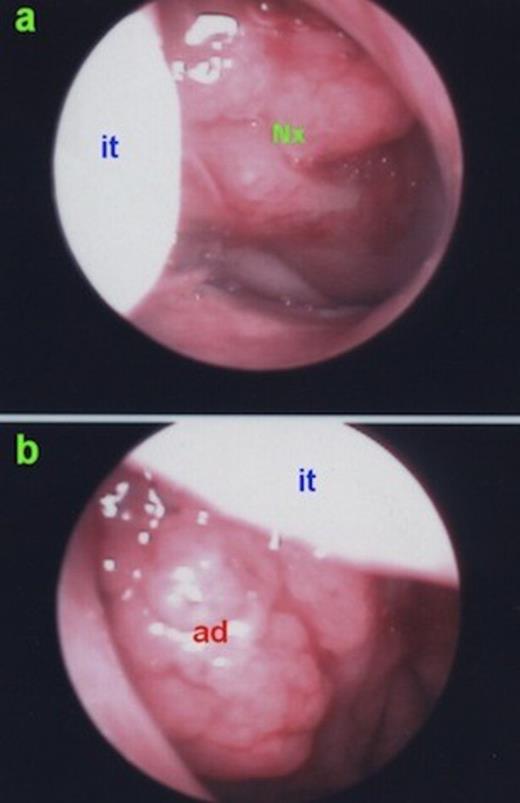
a) Right nasal cavity; clinically insignificant lymphoid hyperplasia on the nasopharynx. b) Left nasal cavity; clinically significant adenoid hypertrophy. it: inferior turbinate, ad: adenoid hypertrophy, Nx: Nasopharynx.
Within the two year follow-up period, the patient is free of any nasal symptoms. Adenoid hypertrophy is not present in the endoscopic nasopharyngeal examination.
DISCUSSION
Rhinolithiasis is a clinical entity caused by rhinoliths (2). Malignant or benign tumors of the nasal cavity may also be calcified (3). The most important differential diagnoses include hemangioma, osteoma, calcified polyps, in the benign tumor category; chondrosarcoma and osteosarcoma in the malignant tumor category; syphilis and tuberculosis in the inflammatory category. CT can provide information that helps to distinguish rhinolith from these entities (3,4). CT also provides information about the accompanying diseases and complications including nasal polyps, septal deviation or sinusitis (5). Rinoliths may be presented as nasal polyps and CT scan is very important in differential diagnosis of these cases (5). Another valuable diagnostic tool is the nasal endoscopy in the differential diagnosis of rhinolithiasis. In a previous report, Ogretmenoglu described the value of endoscopy in the diagnosis of rhinolithiasis (6). However paranasal sinus CT scan, especially in axial slices, would be the preferred method of imaging these masses over endoscopy due to its sensitivity and specificity for calcification and foreign bodies, both important features of rhinoliths. Additionally nasal endoscopy might not be possible to perform on the affected side in case of such a huge space-occupying mass.
The treatment choice of rhinoliths is surgical removal. Endoscopic approach allows the surgeon to intervene accompanying diseases including nasal polyps, sinusitis, septal perforation and septum deviation. Additionally, the surgeon may expose behind the rhinolith by endoscopy. Nasal saline irrigation under direct vision after removal of the rhinolith, was suggested previously in order to prevent revisions (7).
Since chronic inflammation is a common feature of rhinolithiasis, AH may accompany rhinoliths and interfere with nasal obstruction in case of huge-sized rhinoliths. Careful preoperative endoscopic and tomographic examination of nasal cavity generally reveals adenoid tissue. However, as in this case, AH can be asymmetric. Asymmetric adenoid tissue accompanying rhinolithiasis might be overlooked easily and this may cause the symptoms of the patient to persist after the surgery. A careful postoperative endoscopic examination is also mandatory in patients with rhinolithiasis.
This is the first presentation of an asymmetric AH which accompanies rhinolithiasis. However, we have found similar cases in previous reports while reviewing the literature, where asymmetric adenoid hypertrophy was overlooked or underestimated by the authors. In a previous study, a relatively significant asymmetric nasopharyngeal mass was prominent on the axial CT scan of a patient with ipsilateral rhinolith, but the authors did not look any further into this finding (8). In another study, clinically insignificant asymmetric adenoid hypertrophy could be observed on the same side with the rinolith (9).
There are several possible mechanisms for asymmetric AH development in patients with rhinolithiasis. The first suggested mechanism is the persistent inflammation and chronic postnasal drip, which cause chronic low-grade inflammation and interfere with the physiologic regression of adenoid tissue. This mechanism was advocated in a previous report as a cause of persistent adenoid tissue in adults (1). Chronic inflammatory cell infiltration in the adult adenoid tissue also supports this mechanism (1). The second possible mechanism is the nasal obstruction itself. Hamdan et al described the higher prevelance of AH in adults with nasal obstruction than adults without nasal obstruction (10). However, asymmetric AH was not described in this report. The left nasal cavity was totally obstructed in the presented case and lack of airflow in one side might have caused asymmetric AH. Another contribution to this asymmetry might be the lying position of the patient for years. Due to unilateral nasal obstruction, he was lying generally to his left side. Contribution of all these mechanisms with different percentages seems to be the most reasonable mechanism for asymmetric AH in this patient.
As a conclusion, significant asymmetric adenoid hypertrophy may accompany rhinolithiasis. Endoscopic endonasal approach should be the surgical choice unless oroantral fistula is present. Careful endoscopic nasopharyngoscopy as well as paranasal CT scan should be performed before the removal of a rhinolith in order not to overlook asymmetric adenoid tissue. More than one mechanism seems to contribute to the formation or persistance of asymmetric adenoid tissue in the rhinolithiasis patients.

{kind=link}
{kind=link}
{kind=link}