





Abstract
A 51 year old man presented with a short history of severe upper abdominal pain and vomiting. An initial chest radiograph demonstrated gas in the right subphrenic space and a subsequent CT scan demonstrated a hernia through the mid-part of the right hemi-diaphragm, containing small bowel and omentum. A detailed history revealed that there had been trauma to the right side of the chest approximately 12 years previously. An emergency laparoscopy revealed a right sided diaphragmatic hernia containing non-viable small bowel and omentum. After converting to a small midline laparotomy, a small bowel resection and primary anastomosis was performed. The patient was discharged from hospital 12 days later. In any patient presenting with symptoms of upper abdominal pain, with a prior history of trauma, the diagnosis of diaphragmatic hernia should therefore be considered.
INTRODUCTION
Patients are commonly admitted to hospital under the care of the surgical team with upper abdominal pain. This case report highlights the importance of taking a detailed past medical history in order to make an early accurate diagnosis, as what may initially appear to be a common presenting complaint may arise from an uncommon and potentially very serious pathology.
CASE PRESENTATION
A 51 year old previously fit and well man presented to the emergency department with sudden onset of severe epigastric pain and vomiting. The pain was described as sharp and constant, of 3 hours duration, and radiated to his right shoulder. It was unremitting, and he had not experienced it previously, although there was a vague history of a minor road traffic accident approximately 12 years earlier.
On examination he was alert and orientated, although clearly in significant pain. He was tachypnoeic (23rpm) and tachycardic (96bpm). Cardiovascular and respiratory examinations were otherwise unremarkable. His abdomen was soft and not distended but was tender in the right upper quadrant and epigastrium.
Investigations demonstrated a mildly elevated white blood cell count, with the rest of the blood tests normal. An erect chest x-ray showed an area of increased opacification in the right lower zone, with gas in the right subphrenic space which was reported to be Chilaiditi’s syndrome. (Figure 1)

Chest radiograph taken shortly after admssion
An unusual gas pattern was noted in the right lower zone, raising the suspicion of a small bowel diaphragmatic hernia, perhaps through the Foramen of Morgagni. Following initial resuscitation the patient underwent a CT scan. This confirmed a hernia through the mid part of the right hemi-diaphragm, containing omentum and loops of small bowel. (Figure 2)
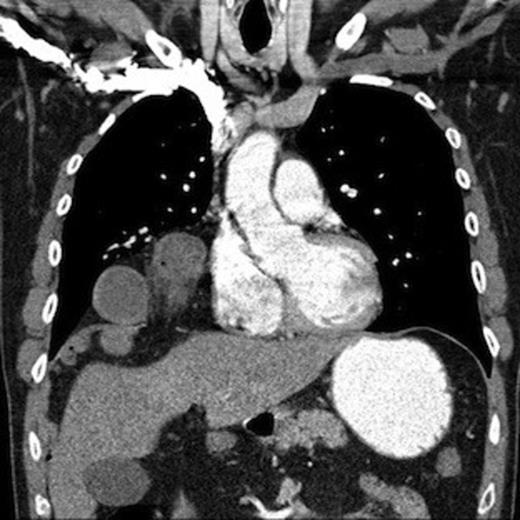
CT scan of chest & abdomen demonstrating diaphragmatic hernia
The patient was taken to theatre, and a 3 port laparoscopy was performed. Initial findings were of dilated small bowel overlying the liver, and a diaphragmatic hernial defect visualised to the right of the falciform ligament. Omentum and small bowel was noted entering the defect. (Figure 3)

Small bowel & omentum seen entering hernial defect
The edges of the hernial defect were enlarged and the small bowel and omentum reduced with difficulty. A segment of approximately 15cm of small bowel and most of the omentum were non-viable. (Figure 4)

Necrotic small bowel removed from chest cavity
The chest cavity was examined via the hernial defect, and no hernial sac was present. The right lung was healthy but collapsed. (Figure 5) In view of the findings, a laparotomy, via a small upper midline incision, was performed. The necrotic segments of bowel and omentum were resected, and a primary anastomosis performed. A 24-gauge chest drain was inserted via the hernial defect, and the diaphragm closed with interrupted 1-nylon sutures. The abdominal incision was closed in layers.
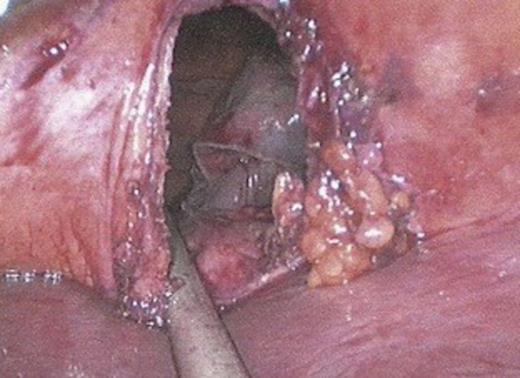
Diaphragmatic hernia defect. The right lung can be visualised through the defect
Post operatively the patient was transferred to ITU for ventilation, and he was successfully extubated the following day and the chest drain removed. Post operative recovery was complicated by a paralytic ileus and persistent right basal consolidation and effusion. The ileus was managed conservatively with normal bowel function returning on day 8. The chest changes resolved with conservative management. The patient was discharged home well on day 13.
DISCUSSION
Diaphragmatic herniae are well described following blunt thoraco-abdominal trauma, with an incidence of up to 5% (1,2). A Medline search revealed only very limited results describing cases with such a delay in diagnosis (3,4), however no such case could be found for a similar strangulated right sided hernia, using a laparoscopic approach to repair.
This case study demonstrates that due to the possible asymptomatic nature of diaphragmatic injuries, the diagnosis can be easily missed or delayed, with potential for serious sequelae, This diagnosis should therefore be considered in any patient with upper abdominal pain and a prior history of trauma. This further highlights the importance of accurate history taking, as patients presenting with what initially appear to be common complaints may actually have an uncommon and potentially serious pathology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}