





Abstract
Cholecystitis can result in complications if not completely treated. These include gallbladder empyema, perforation and cholecystoenteric fistula.
We report the first incidence of cholecystitis resulting in a gallstone fistula with a gastric duplication cyst. A 71 year old patient presented with generalised peritonism that was worst in the epigastric area. Computer tomography (CT) revealed a perforated necrotic gallbladder. Emergency laparotomy, cholecystectomy, partial gastrectomy and Roux-en-Y reconstruction was required. The patient made a slow but full recovery.
Pathology results revealed that chronic cholecystitis had resulted in a fistula with a duplication cyst overlying the greater curve of the stomach. Several one centimeter gallstones were found within the cyst cavity.
INTRODUCTION
Cholecystitis is a common condition that is treated with intravenous antibiotics and often eventually requires the patient to undergo a cholecystectomy. However, if treatment is delayed or incomplete, chronic cholecystitis results in complications that include acute pancreatitis, gallbladder empyema, perforation and cholecystoenteric fistula. Mirizzi’s syndrome is one rare phenomenon in which fistula forms between the gallbladder and large bowel, facilitating entry of the stone into gastrointestinal tract. The fistulous connection usually forms after a preceding episode acute cholecystitis leads to inflammation and adhesions forming between the gallbladder and colon, usually at the hepatic flexure. It is important to be aware of Mirizzi’s syndrome as it is a cause of bowel obstruction.(1) Bouveret syndrome is another rare complication of cholelithiasis with an incidence of 1-3% of those with gallstone ileus.(2) It occurs when a gallstone passes through a cholecystoduodenal fistula and lodges in the pylorus or proximal duodenum causing a gastric outlet obstruction.(3)
We report the first incidence of chronic cholecystitis resulting in a fistula between the gallbladder and a duplication cyst overlying the stomach. The cyst was found to contain several gallstones.
CASE REPORT
A 71 year old obese patient presented with a one day history of epigastric pain that had become generalised, constant and reported as 10/10 severity at its worst. The patient was nauseated but had not vomited. She had no bowel or urinary symptoms. She admitted to having a longstanding heartburn. Further past medical history revealed angina, Type 2 Diabetes Mellitus, asthma, transient ischaemic attacks and atrial fibrillation.
On examination her abdomen was distended, bowel sounds were reduced, she had generalised peritonism that was worst in the epigastric area. Biochemical and haematological investigations revealed a C-reactive protein of 7.4mg/L and a white cell count of 17.6 × 109/L. Liver function tests (Bilirubin 13, alkaline phosphatase 78, alanine aminotransferase 20) and serum amylase were entirely normal.
A CT scan of the abdomen and pelvis was requested which revealed inflammation surrounding the anterior of the stomach, a large irregular thick-walled collection arising from the fundus of the gallbladder, free fluid around the liver, spleen and paracolic gutter. Appearances were consistent with gallbladder perforation.
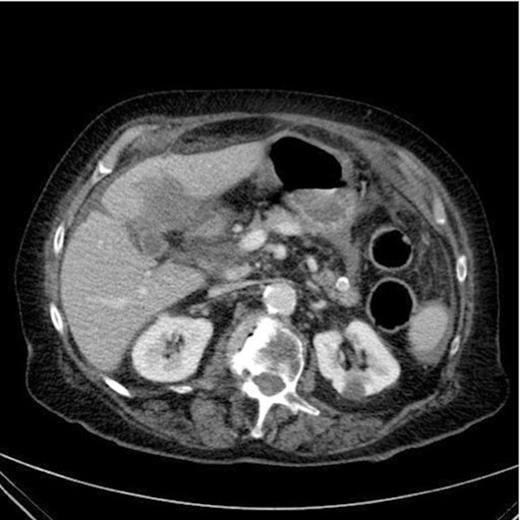
CT Scan demonstrating a thick walled gallbladder with free fluid in the paracolic gutter and a collection in the porta hepatis
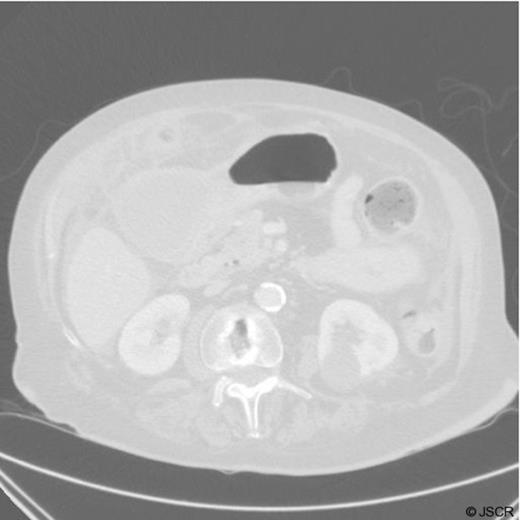
CT Scan demonstrating a gastric duplication cyst
It is unclear from the CT images whether the cyst is contained within the gastric cavity. Malignancy was also a potential concern at this stage.
An emergency laparotomy was undertaken due to the radiological findings and clinical deterioration of the patient. During the operation much purulent fluid was found. The gallbladder was shrunken, thick-walled and fistulated into gastric duplication cyst which contained several one centimetre gallstones and pus. These findings resulted in the patient undergoing a cholecystectomy, partial gastrectomy and a Roux-en-Y reconstruction. A feeding jejunostomy tube was also placed during the operation.
The pathology report confirmed that the gallbladder had features of chronic cholecystitis and the gastric mucosa was consistent with a duplication cyst that did not communicate with the gastric cavity. There was no evidence of dysplasia or malignancy.

Histological specimen demonstrating the cyst overlying the stomach

Specimen demonstrating a gastric duplication cyst in the gastric lining
The patient recovered from the operation in intensive care and then underwent rehabilitation by a multi-disciplinary team on the ward.
DISCUSSION
Gallstone is a common disease with a prevalence of 10% in the United States and Western Europe. However, it is only symptomatic in 20–30% of patients, with biliary pain “colic” being the most common symptom.(4) An accurate diagnosis is essential to the management and prevention of further complications. An abdominal ultrasound scan is a non-invasive tool to detect gallstones, which in addition to blood tests and the clinical impression of the patient can help determine the underlying pathology. Intravenous antibiotics are an important initial treatment, endoscopic retrograde cholepancreatography can then be utilised to remove gallstones, insert stents to aid drainage of the gallbladder and perform sphincterotomy. Endoscopic or extracorporeal lithotripsy and laparoscopic cholecystectomy are further options. If the diagnosis is unclear or more complex CT scans have proved to show better visualisation and are therefore considered to be the gold standard.(5) Appropriate treatment should be implemented after considering the diagnosis and health of the patient.
The presentation reported was acute and required emergency surgery despite multiple co-morbidities. The patient was due to have an elective cholecystectomy after reducing a certain amount of weight. This delay resulted in the development of chronic cholecystitis. The complication that resulted from this ongoing inflammation was a perforated, necrotic gallbladder fistulating with a gastric duplication cyst, which was found to contain multiple gallstones.
Prognosis is frequently related to early recognition, management of any co-morbid conditions, and careful selection of treatment modalities.(4) In conclusion, cholecystitis should be appropriately treated to prevent patients suffering with ongoing symptoms and eventually developing complications that cause them to require urgent higher risk surgery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}