





Abstract
A sixty-one year old man was referred with a history of progressive dysphagia, vomiting and weight loss with some back pain. Upper gastrointestinal endoscopy and biopsies revealed a gastro-oesophageal junction adenocarcinoma. Despite the absence of metastatic disease on computed tomography, positron emission tomography demonstrated multiple vertebral and sternal deposits. He was reviewed in an ENT clinic with a sudden onset of hearing loss accompanied by dizziness, but no focal neurology. Magnetic resonance imaging identified bilateral 2cm lesions at the internal auditory meatus, consistent with a diagnosis of bilateral acoustic neuromas. The patient subsequently died of carcinomatosis and, because of the potential familial significance of bilateral acoustic neuromas, a limited post-mortem examination was carried out. Unexpectedly, this revealed bilateral adenocarcinoma metastases infiltrating the internal auditory meatus affecting the acoustic nerves. The authors believe this a very rare presentation of metastatic gastric disease.
INTRODUCTION
Gastric carcinoma is the 7th most common tumour in the UK, with an incidence of 13 per 100,000 population. Unfortunately, patients often present with evidence of locally advanced or metastatic disease. We present here the unusual case of deafness in a 61 year old man caused by the presence of metastatic gastric adenocarcinoma.
CASE REPORT
A sixty-one year old man presented with a history of progressive dysphagia, vomiting, weight loss and new onset of back pain. Upper gastrointestinal endoscopy revealed a lesion at the gastro-oesophageal junction (figure 1) and biopsies confirmed the presence of adenocarcinoma with signet ring differentiation. Despite the absence of metastatic disease on computed tomography, positron emission tomography demonstrated multiple vertebral and sternal deposits.
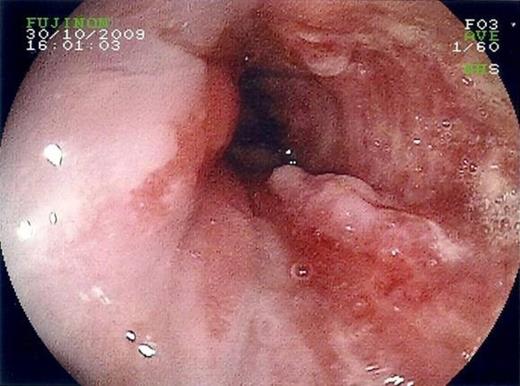
Distal oesophageal adenocarcinoma, viewed on endoscopy.
He developed a sudden loss of hearing which was initially unilateral but became bilateral. The deafness was accompanied by dizziness, but there was no other detectable focal neurology. Magnetic resonance imaging identified bilateral lesions, each approximately 2 centimetres in diameter, at the internal auditory meatus (figure 2), consistent with a radiological diagnosis of bilateral acoustic neuromas.
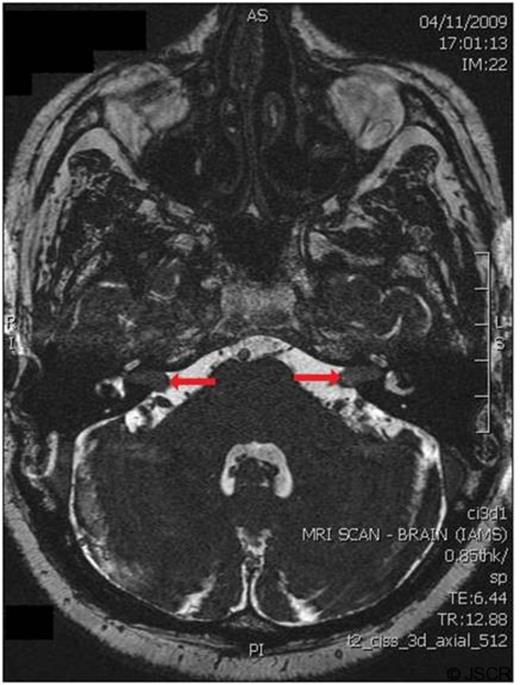
Magnetic resonance imaging at the level of the internal auditory meatus, showing bilateral mass lesions (highlighted by arrows)
The patient subsequently died of carcinomatosis and a limited post-mortem examination unexpectedly revealed bilateral metastatic adenocarcinoma infiltrating the internal auditory meatus and the acoustic nerves (figure 3).
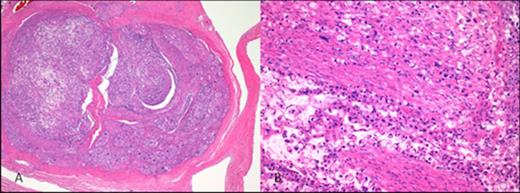
Low power (40x) magnification showing the acoustic nerve within the auditory canal (A), but extensive infiltration with metastatic gastric adenocarcinoma demonstrated on high power (200x) magnification (B). (Haematoxylin and eosin staining after 10% formic acid decalcification)
DISCUSSION
Gastric carcinoma is the 7th most common tumour in the UK, with an incidence of 13 per 100,000 population. Unfortunately, patients often present with evidence of locally advanced or metastatic disease.
In addition to local invasion and regional lymph node metastases, other unusual sites of metastasis include the breast (1), spleen (2), skin (3) and meninges (4). Temporal bone metastases have been reported throughout the literature from numerous different tumours, including renal and bronchogenic carcinomas (5), although it has been suggested that these metastases are often asymptomatic (6). In contradiction to this, a report by Suzuki et al documented four cases of bilateral hearing loss due to metastatic gastric carcinoma, although in three of the four cases the deafness was due to a process different to direct infiltration with metastatic tumour (7).
In this presented case, bilateral internal auditory meatus infiltration with metastatic adenocarcinoma was an unexpected finding. The limited post-mortem was carried out because of the radiological appearance of acoustic neuromas, which could have had a major significance for the patients’ family, given the hereditary nature of type II neurofibromatosis. Although an unusual cause of deafness, reported only once previously to the authors’ knowledge, this case report highlights the unpredictable nature of malignant disease and should serve as a reminder that patients with gastric adenocarcinoma may present with bilateral hearing loss.

{kind=link}
{kind=link}
{kind=link}