





Abstract
Primary liposarcoma of the mediastinum is an uncommon tumour. We report a case of a 45-year-old female who was found incidentally to have a large anterior mediastinal mass. Complete removal of the tumour was accomplished successfully. Appropriate immunohistochimical stains were performed, confirming the presence of a well-differentiated liposarcoma of the mediastinum. We describe an unusual case of a large asymptomatic primary liposarcoma of the mediastinum.
INTRODUCTION
Liposarcoma is a malignant tumour that arises predominantly in the extremities or in the retroperitoneum. Less commonly, it can involve other anatomic sites. The few reported cases of mediastinal liposarcomas illustrate the rarity of this pathology. Patient most commonly present with respiratory symptoms secondary to the compression or local invasion of the tumour or from metastatic spread of the lesion. Surgical resection represents the mainstay of therapy. We report a case in which a large incidentally found primary mediastinal liposarcoma was successfully resected.
CASE REPORT
A 45-year-old female presented with symptoms of gastroesophageal reflux. Her past medical history included hypothyroidism and endometriosis. The patient reported fatigue over several months, but denied any chest pain, fever, dyspnea, cough or weight loss. Physical examination was unremarkable. She underwent a double-contrast upper GI series which revealed no abnormalities in the oesophagus or stomach but was suggestive of an intra-thoracic mass. Chest radiograph noted a heavily calcified mass in the anterior mediastinum. Computed tomography (CT) scan of the thorax revealed a well defined mass of mixed density with speckled calcifications located in the antero-superior mediastinum. The lesion extended from the sternal notch to the level of the aortic root (Figures 1a and 1b). Laboratory tests including β-HCG, α-fetoprotein, CEA, LDH and TSH were all within normal limits and pulmonary function tests were normal. Preoperatively, the working diagnosis was a thymoma, although not typical in appearance, and thus surgical resection was planned. The operation was performed through a median sternotomy. A radical “en-bloc” resection of the tumour, mediastinal fat, thymus, pericardium and pleura was carried out. There was no evidence of tumour dissemination in the pericardium or pleural cavities or metastatic lymphadenopathy. Macroscopically, the tumour was completely resected with negative margins. The patient had an uneventful postoperative course and was discharged one week after surgery. A 24 month follow-up has shown no recurrence of the disease.
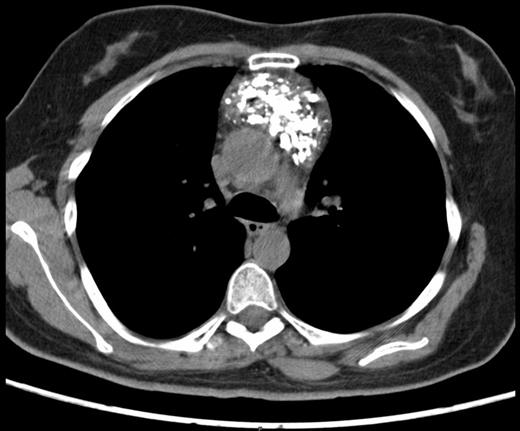
Preoperative chest computed tomography scan revealing a large mediastinal mass - Axial view
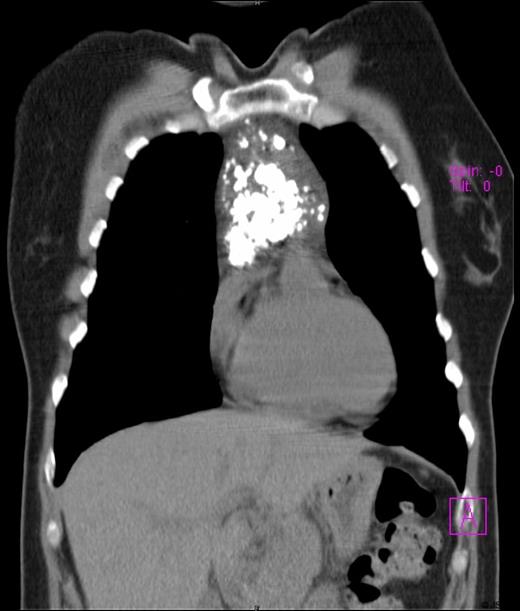
Preoperative chest computed tomography scan revealing a large mediastinal mass - Coronal view
On gross pathologic examination, the mass measured 13 x 9 x 3 cm and weighed 297 grams. Cut section revealed an indurated calcified mass with a lobulated aspect and a whitish coloration. The lesion was well circumscribed but not encapsulated. Microscopically, the tumour was composed of adipocytes of varying sizes including univacuolated and multivacuolated lipoblasts with a large hyperchromatic nucleus (Figure 2). Several fibrous septa containing atypical stromal cells with hyperchromasia were also noted. Immunohistochemistry revealed diffuse and intense tracer uptake for Vimentine, light to moderate uptake of CD34, and a tracer uptake of several fusiform cells and adipose cells with the protein S-100. Based on the above morphological and immunohistochemical characteristics, the definitive diagnostic was consistent with a well-differentiated liposarcoma (atypical lipomatous tumour). There were no features of dedifferentiation.
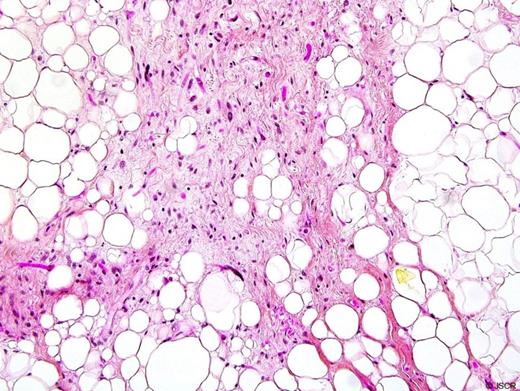
Histological examination of the mass showing adipocytes of varying sizes including univacuolated and multivacuolated lipoblasts with a large hyperchromatic nucleus.
DISCUSSION
Liposarcoma is the most common of all soft tissue sarcomas, representing approximately 20 % of all mesenchymal malignancies (1). Less than 5 % of liposarcomas occur in the mediastinum. Primary mediastinal liposarcoma is infrequent and accounts for less than 1 % of mediastinal tumors. The mean age of primary mediastinal liposarcoma has been reported to be 51-year-old (2).
Generally, mediastinal liposarcoma is not identified at an early stage but rather when the tumor has become large and causes symptoms due to invasion or compression of adjacent structures such as the heart, great vessels or lungs. When present, symptoms typically include dyspnea, tachypnea, wheezing and chest pain (3-5). Rarely, as in our patient, it can be discovered incidentally by radiological imaging in an asymptomatic patient.
Imaging characteristics are variable. The most common radiographic feature of mediastinal liposarcoma is a widened mediastinum. Computed tomography (CT) scan findings can provide helpful information regarding the fat-containing nature of the mass. However, differentiation from other tumors (including thymoma) arising from the mediastinum remains difficult. The consistency of the tumor can vary from a major fatty aspect to a solid mass (5,6). In the present case, the most probable preoperative diagnosis was a thymoma. The definitive diagnosis of liposarcoma cannot be established with certainty by noninvasive methods and thus an open biopsy is generally required (4).
Liposarcoma varies in histologic patterns and can be classified into subtypes: well differentiated, myxoid, round cell type pleomorphic, and dedifferentiated. Differential histologic diagnosis can be difficult and further analyses are required. Liposarcoma seems to appear in equivalent occurrence in the anterior and posterior mediastinum. For the most part, mediastinal liposarcomas are well-differentiated (1,2).
Dedifferentiated and pleomorphic liposarcomas have a propensity to be more aggressive and have a less favourable prognosis with regards to local recurrence and distant metastasis than well-differentiated liposarcoma. Location and size of the tumour are important prognostic factors because they help establish the possibility of carrying out a complete resection (2,3). Complete surgical excision is the primary treatment modality (1-8) and currently, there is no definitive evidence to support adjuvant therapy. (7,8) Surgical resection combined with post-operative radiation therapy is a commonly used modality. In our case, considering the close margins and the risk of local recurrence, external beam radiotherapy was recommended but refused by the patient.
In conclusion, liposarcoma of the mediastinum is a rare malignancy that is best managed by complete surgical removal. Its clinical and radiological presentation is variable and can mimic a number of other pathologies. The risk of recurrence is related to the completeness of the resection as is the case with most sarcomas. Prognosis is also affected by the tumour subtype and differentiation. Although not established, the use of adjuvant therapy continues to be explored.

{kind=link}
{kind=link}
{kind=link}