





Abstract
Carpeted villous adenomas of rectum may be extensive and not suitable for transanal excision or Endoscopic mucosal resection. We present a case of such lesion extending from anorectal junction to rectosigmoid region. After biopsy and staging, this was managed by a sphincter saving procedure, i.e. a combination of transabdominal total mesorectal excision and transanal intersphincteric dissection, with acceptable functional outcome with 8 years of follow up.
Introduction
Carpeted villous adenomas of rectum may be extensive and not suitable for transanal excision or Endoscopic mucosal resection. We present here the case of a 69 years old lady presenting with 6 months history of diarrhoea, urgency of defecation and rectal bleeding.
Case Report
A 69 years old lady presented with 6 months history of diarrhoea, urgency of defecation and rectal bleeding. Digital rectal examination revealed soft to firm polypoid lesion in the rectum.
Flexible sigmoidoscopy, revealed a 35 mm sessile polyp in the rectum just above the dentate line, associated with diffuse field changes from lesion to rectosigmoid junction (fig 1). The biopsy of the polyp as well as the field changes was reported as tubular adenomatous polyp with mild to moderate epithelial dysplasia. A check colonoscopy revealed no other lesion in the rest of colon.
Red Carpet of the rectum
CT scan was preformed which showed the rectum to be quite distended and thick walled. MRI showed that the lesion to be confined to rectal mucosa.
The patient underwent surgery in the form of ultra low anterior resection and hand-sewn colo-dentate anastomosis.
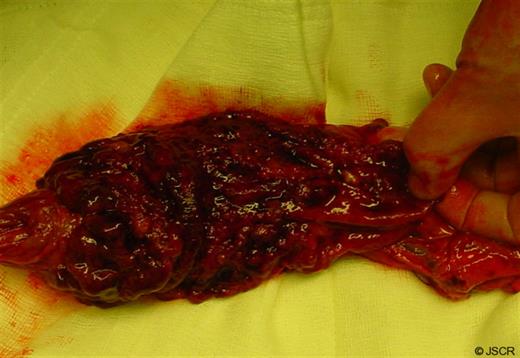
A laparotomy with mobilisation of the left colon and the rectum was followed by formation of a colonic pouch. The perineal part of the operation was facilitated by placement of the lone star retractor, mucosal incision 1 cm above the dentate line, division of the internal anal sphincter 2 cm above the mucosal incision followed by intersphincteric dissection and transanal disconnection of specimen at the level of the anorectal junction. A handsewn coloanal anastomoses along with a defunctioning ileostomy was performed (fig 2). Histologic examination of the speciman showed a very large villous adenoma with focally up to severe dysplasia with no evidence of invasion of the lamina propria. All ten lymph nodes identified and they were negative. Post operative course was uneventful. Contrast enema performed 4 months later showed intact anastomosis and the ileostomy was reversed. Eight years after the operation she has acceptable function (CCS score of 5) and quality of life (McMaster quality of life).
Discussion
Adenomatous polyps, the most common type of colorectal polyps do have a malignant potential and they are classified into tubular (67%), villous (5%) and tubulovillous (8%) polyps, villous adenomatous polyps have the highest malignant potential. (1)
Malignant potential dramatically increases with size. In Morson’s series of 2499 tubular and villous adenomas, the incidence of carcinoma in polyps less than 1 cm in diameter was 1.3%; in polyps 1-2 cm in diameter, 9.5%; and in polyps over 2 cm in diameter, 46%. (2)
Carpet lesions of the colon were first described using double-contrast barium enema by Rubesin et al.(2) and were defined as flat, lobulated lesions causing an alteration in surface texture. They often involve a large surface area of the colon with little or no protrusion into the lumen. Carpet lesions have been recognized as a separate entity from flat adenomas, flat depressed adenomas, and plaque like carcinomas. Carpet lesions have been grouped with villous tumours, given their propensity to contain villous components. The prevalence of carpet lesions is uncertain and, to our knowledge, has not been reported; Carpet lesions occur predominantly in the caecum, ascending colon, and rectum for reasons that are not well understood. (2,3) These lesions may also be seemingly indistinguishable from the normal surrounding colonic mucosa on colonoscopy. (4)
While they may present with lower GI symptoms, hypersecretory diarrhoea and electrolyte abnormalities (Mckittrick- Wheelock syndrome) have been reported. (5)
Given the large size of carpet lesions, it is somewhat difficult to completely examine the entire lesion for malignant foci with biopsies alone. Although their malignant degenerative potential is unclear, small series report malignancy rates of 7-40%. Thus, surgical resection is currently the recommended treatment for all carpet lesions. (4) For unfit patients not amenable to EMR, argon plasma coagulation may be attempted but with no long term available results.
Differential diagnosis of diffuse lesions can include endometriosis, proctitis, and submucosal spread of a tumour or rare cause like Yersinia enterocolitica, herpetic infection, ischemia, and Crohn’s disease. (2)
The treat of such carpeted lesions in low rectum can be APER or sphincter saving ultralow anterior resection and hand sewn low colo-anal anastomosis. Our patient had clinically good sphincter function and was keen on sphincter preservation. This achieved acceptable outcome.

{kind=link}