





Abstract
Urethral injuries in females are rare, and the literature describes various surgical techniques to manage these cases. However, the reported cases were managed with open surgery. We present a case of complete loss of urethra managed using three-dimensional laparoscopy. The patient had a recent history of vaginal hysterectomy complicated by post-operative retention. Multiple urethral dilatations were performed which ultimately stopped working and the patient presented to us in a state of chronic retention. Multiple investigations including an examination under anaesthesia, micturating cystourethrogram, and surgical trans-vaginal exploration confirmed the absence of a meaningful urethra, and the patient was planned for a neourethral reconstruction. This was performed using three-dimensional laparoscopy. The neourethra was created using an anterior bladder flap. At 12 months follow-up, the patient has normal continence and voids to completion. Laparoscopic urethral reconstruction can yield good functional results and offers the known benefits of minimally invasive surgery.
Introduction
Urethral injuries in females can result in partial or complete loss of urethra. Various surgical techniques are described in literature to manage this but there is no consensus regarding an optimal approach. We describe a case of complete loss of urethra which was managed with three-dimensional (3D) laparoscopic neourethral reconstruction. To the best of our knowledge, this is the first report in literature to describe the use of this technique laparoscopically.
Case report
Patient history
A 57-year-old female (Fig. 1) who developed post-operative urinary retention following a hysterectomy. She was initially catheterized but experienced difficulty voiding following catheter removal. Repeated urethral dilatations were performed, with temporary improvement in voiding. Ultimately, the dilatations became unsuccessful, and the patient presented with chronic urinary retention.
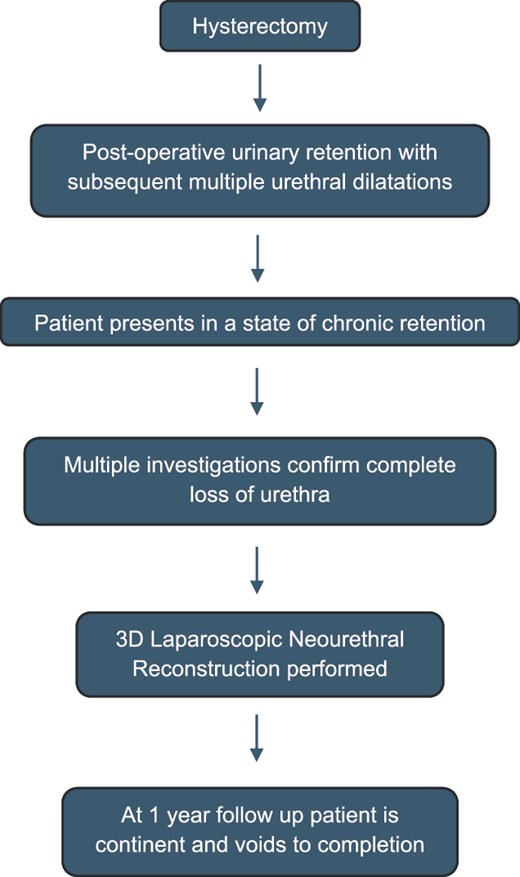
Summarized timeline of the patient’s journey from presentation to follow-up.
Investigations
Following supra-pubic catheterization (SPC), a micturating cystourethrogram was performed, which demonstrated no recognizable urethra, with failure of bladder neck opening. There was no identifiable external urethral meatus (EUM) on examination under anaesthesia and antegrade cystoscopy through the SPC track revealed a blind pit at the site of the bladder neck. A trans-vaginal exploration of the mid-urethra demonstrated a fibrous, cord-like structure, but no meaningful urethra. Hence, complete loss of urethra was diagnosed.
Operative technique
3D laparoscopy was used and 3D goggles were worn by surgical team members. 3D visualization significantly improves depth perception allowing for precise and efficient surgical manoeuvres.
The patient was positioned in lithotomy with 30 degrees Trendelenburg and five port (11 mm ×2, 5 mm ×3) transperitoneal access gained.
The SPC catheter was pulled out partially, and the SPC track was disconnected. The balloon was inflated in the SPC track to prevent CO2 leak.
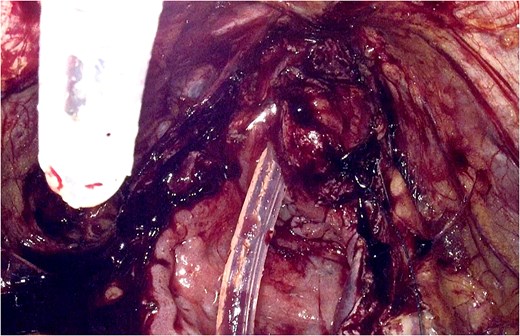
The bladder was opened and the absence of a viable urethra was reconfirmed. A pit was visible at the bladder neck (Fig. 2).
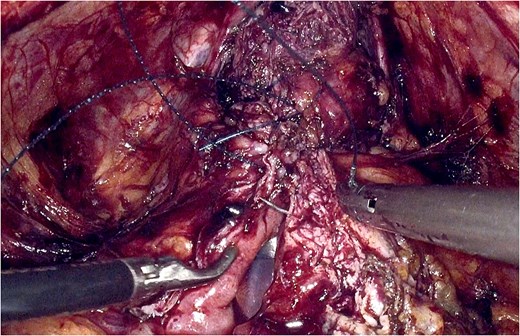
A 2.5 cm wide and 4.5 cm long bladder flap was raised, with its base anterior to the native bladder neck (Fig. 3).
The flap was tubularized using 3-0 V-loc suture, forming a neourethra.
A tongue-shaped flap was created anterior to the native EUM. Aided by blunt artery forceps, a tract was created through the perineal muscles to reach the retropubic space (Fig. 4).
The neourethra was held using forceps by way of a stay suture and pulled through, to the previously raised tongue flap.
The tongue flap was fed into the spatulated distal end of the neourethra, and the remaining margins of the neourethra were sutured to the vestibular mucosa to create the neo-EUM.
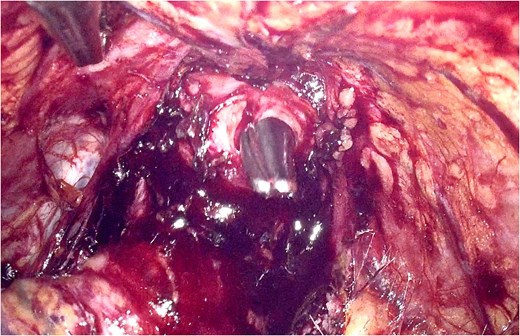
An 18Ch silicon catheter was placed through the neourethra (Fig. 5).
The SPC was reinserted, and the bladder was closed in two layers using 3-0 V-loc suture (Fig. 6).
A 3 mm suction drain was placed in the pre-vesical space, and ports closed in standard fashion.
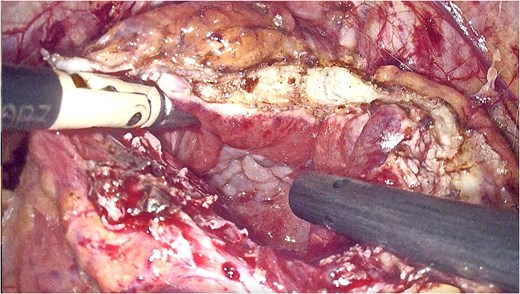
Laparoscopic view of the blind pit at the site of the native bladder neck.
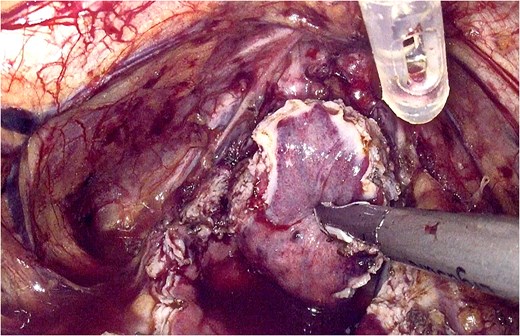
Laparoscopic view of the raised bladder flap.
Laparoscopic view of the tract created by blunt artery forceps through the perineal muscles.
Laparoscopic view of the catheter placed through the neourethra prior to closure of the bladder.
Laparoscopic view of the final layer of bladder closure.
Important considerations
To minimize the risk of fistula formation, all suture lines in the bladder and the neourethra were anterior. Moreover, the urine was diverted via SPC for an adequate period of time. To minimize the risk of stricture formation, meticulous dissection of the tissues with gentle handling was performed to ensure good preservation of the vascular supply. Maintaining good vascularity and using an appropriate width to length ratio helped ensure long-term viability of the bladder flap.
Post-operative management and follow-up
Two weeks post-operatively a cystogram with post-evacuation films revealed no bladder leak and the urethral catheter was removed. The SPC was clamped to enable a trial of voiding. The patient was able to void and maintain continence. After a further 2 weeks, minimal post-void residual volumes were demonstrated and the SPC was removed. The patient has been followed up for 12 months. Repeat uroflowmetry demonstrated a bladder capacity of 377mls and post-void residual volume of 38mls. The patient reported an ICIQ-LUTSqol score of 32/76 indicating a good quality of life.
Narrative review and discussion
Urethral injuries in females are rare [1]. Causes include trauma from pelvic fractures, prolonged/obstructed labour, anterior vaginal or urethral surgery, urethral catheterization, and pelvic irradiation [2, 3]. While neourethral reconstruction is possible, maintaining or restoring voiding function and continence is challenging [4]. A variety of techniques exist for urethral reconstruction [5, 6]. Few cases in the literature describe repair of an entirely obliterated urethra. Radwan et al. performed a Tanagho bladder tube in 6 patients with total urethral loss. Complete continence was achieved in 4 patients, and partial continence achieved in 1 [7]. Sawant et al. used a tubularized anterior vaginal flap for reconstruction of total urethral loss in seven patients. Of these, 86% achieved full continence, while 14% had mild incontinence following the procedure [8]. Another study described 3 paediatric cases with traumatic complete loss of urethra managed with bladder flap reconstruction but all patients had some degree of incontinence [9]. Adaptations to the Tanagho technique have been attempted to improve functional outcomes. Nayyar et al. incorporated wrapping of omental tissue around the urethral anastomosis, to protect the neourethra from tethering to the pubic bone, as well as anteriorly placed sutures to prevent formation of a fistula [10]. They reported normal continence and voiding post-operatively [10].
The key difference between reported cases and ours is the use of laparoscopy, facilitating quicker post-operative recovery, reduced pain, and better cosmesis [11]. All other cases described in literature were performed using open surgery [7, 9, 10]. We placed anterior sutures to secure the flap as Nayyar et al. described [10]. However, the neourethra was not sutured to the native EUM. Instead, a neo-EUM was formed, and an entirely new urethra was created. This distinguishes our technique from the classic Tanagho tube repair where the neourethra is anastomosed with the distal native urethra.
It is challenging to comment on optimal surgical technique due to paucity of literature. Decisions about the appropriateness of intervention should consider patient factors, the nature of the injury and availability of surgical expertise.
Conclusion
To our knowledge, we have described the first laparoscopic neourethral reconstruction for iatrogenic total loss of urethra. The use of laparoscopy improves patient morbidity, and the functional outcome is comparable to that in the literature.
Author contributions
Conception: BSV; Data Acquisition and Literature Review: LEB, YV; Manuscript Writing: LEB, YV; Manuscript Corrections: BSV, SCD; Manuscript Approval: All Authors.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}