





Abstract
A cystic duct entering the right hepatic duct is a rare biliary anatomical variation that increases the risk of bile duct injury during laparoscopic cholecystectomy. We report a 42-year-old woman with cholelithiasis and gallbladder adenomyomatosis in whom preoperative magnetic resonance cholangiopancreatography demonstrated the cystic duct entering the right hepatic duct. During laparoscopic cholecystectomy, the cystic duct ran cranially toward the hepatic hilum and appeared to continue beneath the serosa of the hepatoduodenal ligament into the right hepatic duct. Intraoperative cholangiography confirmed the anomalous anatomy, and the operation was completed safely. The postoperative course was uneventful. A cranially coursing cystic duct and subserosal continuity toward the hepatic hilum may serve as practical intraoperative warning signs of this rare anomaly and should prompt confirmation of biliary anatomy before duct division.
Introduction
Biliary anatomical variations are a well-recognized cause of bile duct injury during laparoscopic cholecystectomy, most commonly because of misidentification of anatomical structures. Among these variations, a cystic duct entering the right hepatic duct is rare, with a reported incidence of ~0.7% [1], and poses a particularly high risk of major bile duct injury if unrecognized. Although preoperative magnetic resonance cholangiopancreatography can facilitate diagnosis, intraoperative recognition remains critical for preventing surgical complications. However, specific intraoperative findings suggesting this anomaly have not been well described. We report a case successfully managed by laparoscopic cholecystectomy, emphasizing visual warning signs that may contribute to safer surgical procedure.
Case report
A 42-year-old woman was referred to our hospital for treatment of cholelithiasis. Abdominal ultrasonography revealed multiple gallstones with acoustic shadowing in the gallbladder. Contrast-enhanced computed tomography (CT) demonstrated numerous calcified stones within the gallbladder and wall thickening at the gallbladder neck (Fig. 1). The patient had a body mass index of 21.0 kg/m2. Preoperative laboratory tests showed aspartate aminotransferase 22 U/l, alanine aminotransferase 21 U/l, alkaline phosphatase 77 U/l, gamma-glutamyl transferase 93 U/l, and total bilirubin 0.63 mg/dl.
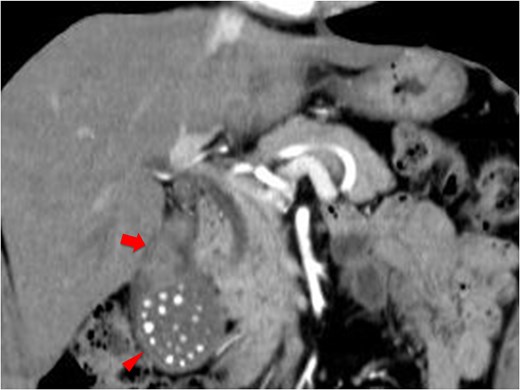
Contrast-enhanced CT (coronal view) showing multiple small calcified stones in the gallbladder (arrowheads) and wall thickening at the gallbladder neck (arrow).
Magnetic resonance imaging revealed small cystic structures within the gallbladder neck wall, consistent with segmental-type adenomyomatosis. In addition, serial coronal T2-weighted images and magnetic resonance cholangiopancreatography demonstrated that the cystic duct drained into the right hepatic duct (Fig. 2).
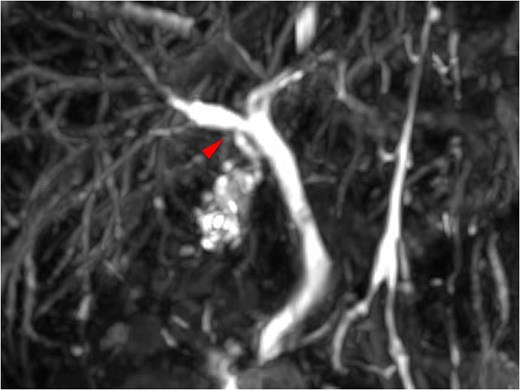
Magnetic resonance cholangiopancreatography showing the cystic duct entering into the right hepatic duct (arrowhead).
During the preoperative conference, the biliary anatomy was shared among the surgical team. As there were no signs of inflammation and the cystic duct appeared sufficiently long, it was considered feasible to manage the cystic duct using standard clips; therefore, prophylactic endoscopic nasobiliary drainage was not performed. However, given the presence of a rare biliary anatomical anomaly, intraoperative cholangiography was planned.
Laparoscopic cholecystectomy was performed. The gallbladder showed no signs of inflammation, and no wall thickening was observed. Dissection was carried out on the ventral side of the Rouviere sulcus along the inner layer of the gallbladder subserosa according to previously reported safe surgical principles [2, 3]. After establishing the critical view of safety (Fig. 3), the cystic artery was divided. The cystic duct was observed running cranially toward the hepatic hilum, which was atypical compared with the usual course toward the common bile duct. This unusual course raised suspicion of an anomalous biliary anatomy. Under laparoscopic magnification, the cystic duct appeared to continue beneath the serosa of the hepatoduodenal ligament into a bile duct presumed to be the right hepatic duct (Figs 4 and 5). A catheter was inserted through the cystic duct, and intraoperative cholangiography confirmed that the cystic duct drained into the right hepatic duct (Fig. 6). The cystic duct was then clipped, and the operation was completed. The operative time was 87 minutes, and the estimated blood loss was minimal.
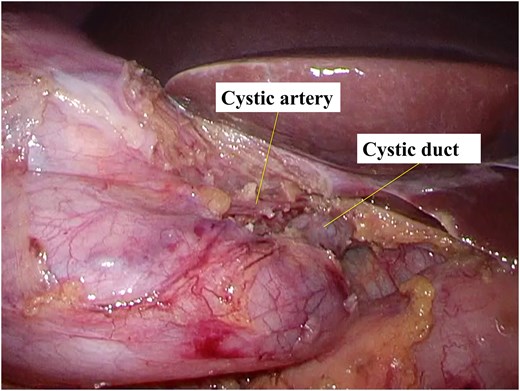
Intraoperative view demonstrating the establishment of the critical view of safety.
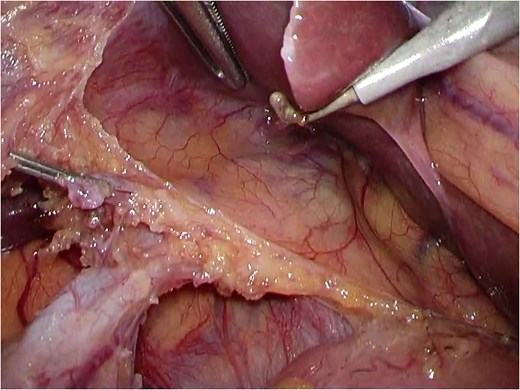
Intraoperative view showing the cystic duct running toward the hepatic hilum and appearing to continue beneath the serosa of the hepatoduodenal ligament into a bile duct presumed to be the right hepatic duct.
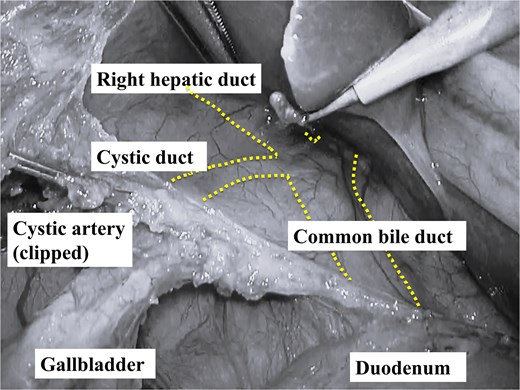
Annotated schematic illustration of the findings shown in Fig. 4, with lines and labels indicating the anatomical structures.
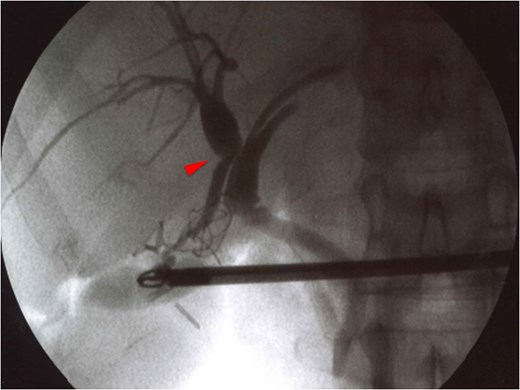
Intraoperative cholangiography demonstrating the confluence of the cystic duct and the right hepatic duct (arrowhead).
The postoperative course was uneventful, and the patient was discharged on postoperative day 4 without complications. Multiple stones were found in the resected gallbladder. Histopathological examination revealed adenomyomatosis at the gallbladder neck, with no evidence of malignancy.
Discussion
Biliary anatomical variations are an important cause of bile duct injury during laparoscopic cholecystectomy. A cystic duct entering the right hepatic duct may lead to misidentification of the right hepatic duct as the cystic duct, resulting in inadvertent clipping or transection of a major bile duct. Previous studies have shown that most bile duct injuries during laparoscopic cholecystectomy are attributable to misinterpretation of biliary anatomy rather than technical failure [4, 5]. Therefore, surgeons must remain alert to anatomical variations throughout dissection.
Preoperative evaluation of biliary anatomy is essential. CT is routinely performed, but it often fails to delineate the cystic duct course. In contrast, magnetic resonance cholangiopancreatography provides a reliable and noninvasive method for visualizing the biliary tree [6, 7]. In the present case, magnetic resonance cholangiopancreatography clearly demonstrated the anomalous drainage, allowing us to anticipate the risk and plan intraoperative cholangiography. The absence of acute cholecystitis, no gallbladder wall thickening, minimal inflammatory change, and a sufficiently long cystic duct supported laparoscopic completion without preoperative biliary drainage.
To clarify the clinical significance of this case, we searched PubMed using combinations of the following terms: “cystic duct,” “entering,” “insertion,” “right hepatic duct,” and “cholecystectomy.” Only a limited number of cholecystectomy cases involving this anomaly were identified [8–15]. Previous reports mainly emphasized preoperative diagnosis, intraoperative cholangiography, preoperative biliary drainage, or subtotal cholecystectomy in difficult cases. In contrast, specific laparoscopic visual findings suggesting this anomaly have rarely been described.
The main educational value of this case is the identification of two intraoperative visual clues. First, unlike the normal cystic duct, which courses caudally toward the common bile duct, the cystic duct ran cranially toward the hepatic hilum. Second, it appeared to continue beneath the serosa of the hepatoduodenal ligament into the right hepatic duct. We propose that a cranially coursing cystic duct and subserosal continuity toward the hepatic hilum may serve as practical warning signs of this anomaly.
Recognition of these findings may prompt surgeons to reassess biliary anatomy and perform intraoperative cholangiography before dividing the cystic duct, even after the critical view of safety has been established. This point is important because the anomaly may not always be recognized preoperatively, and an uncomplicated operative field may lead surgeons to underestimate its significance. When the cystic duct course appears atypical, no ductal structure should be divided until the anatomy has been confirmed.
This report is limited by its single-case nature, and the reproducibility of these findings requires further validation. In addition, the proposed visual signs may not be applicable in all clinical settings. In particular, subserosal continuity of the cystic duct toward the hepatic hilum may be difficult or impossible to recognize in patients with acute cholecystitis or severe chronic inflammation because of inflammatory thickening, edema, or adhesion around the hepatoduodenal ligament. Nevertheless, in patients without severe inflammation, careful attention to the direction and subserosal course of the cystic duct may help surgeons recognize this rare anomaly intraoperatively and avoid bile duct injury during laparoscopic cholecystectomy.
Acknowledgments
Not applicable.
Author contributions
MT collected and analyzed the data and drafted the manuscript. HH and HS provided critical revision and intellectual input. HT, YY, TH, Y Kimura and Y Kumagai contributed to patient management and data acquisition. HH, HS and HY supervised the study and critically revised the manuscript. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Conflicts of interest
None declared.
Funding
None declared.
Data availability
The datasets supporting the conclusions of this article are included within the article.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Japan Community Health Care Organization Utsunomiya Hospital (approval number: 69).
Declaration of generative AI in scientific writing
The authors used an AI-based language editing tool to improve the readability of the manuscript. The authors take full responsibility for the content.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}