





Abstract
Pancreas divisum, a congenital failure of fusion between the dorsal and ventral pancreatic buds, occurs in ~10% of the population. The prevalence of intraductal papillary mucinous neoplasm (IPMN) of the ventral duct in pancreas divisum is not well established. Malignant transformation is exceptionally rare, with this case being the first documented in the USA. A 74-year-old man presented with new-onset obstructive jaundice. A computed tomography of the abdomen and pelvis showed pancreas divisum with a 4-cm cystic mass causing a 1.8 cm ventral pancreatic duct dilatation, concerning for an IPMN. Cyst fluid analysis demonstrated elevated fluid amylase and carcinoembryonic antigen. Due to high-risk stigmata, the patient underwent a Whipple procedure and was found to have a 3.5-cm pancreatic cancer arising from an IPMN of the ventral duct. Given the risk of progression, patients with pancreas divisum who develop ventral duct IPMN require careful surveillance and timely escalation of care when appropriate.
Introduction
The ventral pancreatic bud gives rise to the main duct of Wirsung which will merge with the common bile duct and allow biliary and pancreatic secretions to flow through the major papilla. In 43% of patients, the proximal dorsal pancreatic bud does not degenerate and instead results in a patent accessory duct of Santorini with drainage into the minor duodenal papilla [1]. The ventral and dorsal pancreatic buds fuse by the seventh week. Failure of fusion leads to the common congenital anomaly known as pancreas divisum, seen in ~10% of the population [2]. As a result, the dorsal duct becomes the main draining duct through the minor papillae.
Intraductal papillary mucinous neoplasm (IPMN) is a mucin-producing cystic neoplasm that can occur in the main duct (MD-IPMN), branch duct, or mixed. The 2024 International Consensus Kyoto guidelines have widely been accepted for work-up and management for IPMN [3]. The malignancy potential for MD-IPMN has been documented to be 61.6% (36%–100%), and surgical resection has been shown to improve survival for these patients [4]. The ideal target is high-grade dysplasia prior to malignant transformation [5]. To our knowledge, we present the first reported case of IPMN-derived pancreatic cancer of the ventral duct in a pancreas divisum patient in the USA.
Case report
A 74-year-old man with uncontrolled Type 2 diabetes mellitus with recent history of 20-pound weight loss was admitted to a community hospital after presenting with 3 days of persistent vomiting. Initial laboratory work-up showed transaminitis and elevated bilirubin, consistent with obstructive jaundice, as shown in Table 1.
Laboratory findings.
| Parameter | Patient’s value | Reference range |
|---|---|---|
| Serum sodium | 138 mmol/l | 135–145 mmol/l |
| Serum potassium | 3.7 mmol/l | 3.5–5.0 mmol/l |
| Serum creatinine | 1.34 mg/dl | 0.7–1.3 mg/dl |
| Fasting blood glucose | 342 mg/dl | 70–99 mg/dl |
| Alkaline phosphatase | 223 U/l | 44–147 U/l |
| Aspartate aminotransferase | 72 U/l | 10–40 U/l |
| Alanine aminotransferase | 216 U/l | 7–56 U/l |
| Lipase | 15 U/l | 0–160 U/l |
| Total bilirubin | 2.4 mg/dl | 0.1–1.2 mg/dl |
A right upper quadrant ultrasound revealed gallstones in the gallbladder lumen, obscured ampulla, and intra- and extrahepatic bile duct dilatation. Computed tomography (CT) of the abdomen and pelvis with Intravenous (IV) contrast showed a 3-cm cystic low-attenuation mass within the pancreatic head, abrupt tapering of the intrapancreatic common bile duct with associated dilation of the intra- and extrahepatic bile duct, as shown in Fig. 1a. Subsequent magnetic resonance imaging (MRI) of the abdomen with and without contrast, as seen in Fig. 1b, showed a non-dilated dorsal duct measuring <2 mm throughout, crossing anterior to the common bile duct and terminating at the minor papilla, compatible with pancreas divisum. Additionally, there was a dilated ventral pancreatic duct, up to 1.8 cm, concerning for an IPMN of the ventral duct.
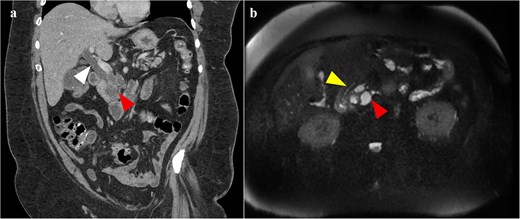
(a) CT of the abdomen and pelvis, seen on the imaging on the left, showing a cystic lesion within the uncinate process of the pancreas (red arrow) with associated biliary dilatation (white arrow); (b) T2-weighted MRI of the abdomen, seen on the imaging on the right, showing markedly hypertense cystic lesion within the uncinate process (red arrow); there is no dilation of the dorsal pancreatic duct (yellow arrow) that does not communicate with this cystic lesion and drains into the minor papillae.
The patient was transferred to a tertiary care center for further work-up and management. The patient underwent endoscopic retrograde cholangiopancreatography with biliary sphincterotomy and covered metal stent placement in the common bile duct. Upper endoscopic ultrasound showed fish-mouth appearing papillae with mucinous discharge, as well as an 11-mm cystic lesion seen in the pancreatic head with a dilated ventral pancreatic duct. Cyst fluid analysis of the cyst showed elevated amylase and carcinoembryonic antigen (CEA). These findings were concerning for an MD-IPMN of the ventral duct, warranting surgical resection.
The patient underwent surgical intervention with pancreaticoduodenectomy. The patient went to the intensive care unit post-operatively for expected management. The hospital course was complicated by pneumonia and a Grade B pancreatic leak. Th patient was discharged on post-operative day (POD) #21. Final pathology showed a 3.5-cm invasive moderately differentiated pancreatic adenocarcinoma arising in association with a pancreaticobiliary-type IPMN with high-grade dysplasia within the ventral pancreatic duct, as illustrated in Fig. 2. Eighteen out of 18 regional lymph nodes were negative for tumor. There was no lymphovascular or perineural invasion. Resection margins were negative for dysplasia or invasive carcinoma. The final classification of the tumor was T2N0M0, consistent with Stage IB pancreatic cancer. The patient received adjuvant systemic chemotherapy with capecitabine and gemcitabine. The patient was seen 12 months post-operatively for follow-up which the patient reported no issues.
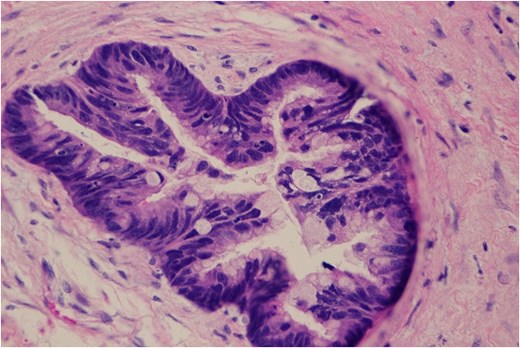
Histological image (×400) of invasive pancreatic cancer arising from IPMN within the uncinate process.
Discussion
IPMN arising in the setting of pancreas divisum is uncommon. One retrospective study reported that ~5.1% of patients with pancreas divisum were diagnosed with IPMN [6]. IPMNs originating from the ventral duct in this anatomic variant are even rarer. Malignant transformation of ventral duct IPMN in pancreas divisum has not been previously documented in the USA.
As noted in Table 2, eight cases of ventral duct IPMN in patients with pancreas divisum have been previously reported worldwide [7–14]. Four patients presented with clinical evidence of pancreatitis. This is a common manifestation in pancreas divisum due to preferential drainage through the minor papillae rather than the major papillae. Our patient is the first documented case that presented with obstructive jaundice. Only one other case from Japan noted malignant transformation.
Cases involving ventral duct IPMN in patients with pancreas divisum based on literature review.
| Authors, year | Age (years)/gender | Pancreatitis | Obstructive jaundice | Location of the IPMN | Invasive carcinoma | Surgery |
|---|---|---|---|---|---|---|
| Sakate et al. 2004 [7] | 34/M | Yes | No | Ventral duct | Absent | Pylorus-preserving pancreatoduodenectomy |
| Santi et al. 2010 [8] | 74/F | No | No | Ventral duct | Unknown | None |
| Gurram et al. 2014 [9] | 39/F | Yes | No | Ventral duct | Absent | Pancreatoduodenectomy |
| Nishi et al. 2015 [10] | 77/F | No | No | Ventral duct | Yes | Pylorus-preserving pancreatoduodenectomy |
| Baiocco et al. 2016 [11] | 70/M | No | No | Ventral duct | Absent | Pylorus-preserving pancreatoduodenectomy |
| Sanchez-Acedo et al. 2019 [12] | 78/M | No | No | Ventral duct | Unknown | None |
| Azad et al. 2023 [13] | 62/F | Yes | No | Ventral duct | Unknown | None |
| Agudo Castillo et al. 2024 [14] | 75/M | Yes | No | Ventral duct | Unknown | None |
| Our case | 74/M | No | Yes | Ventral duct | Yes | Pancreatoduodenectomy |
Clinicopathologic features are noted including the presence of obstructive jaundice and malignant transformation.
Ventral duct IPMN in pancreas divisum patients presents unique diagnostic challenges. Due to the altered pancreatic ductal anatomy, ventral duct IPMN may be overlooked, as imaging and endoscopic evaluation often focus on the dominant ductal drainage. This underscores the importance of high-quality cross-sectional imaging and careful interpretation of imaging and diagnostic modalities when evaluating a patient with pancreas divisum and ventral duct dilatation [15].
Although ventral duct IPMNs in pancreas divisum are rare, management should follow established IPMN guidelines [3]. Patients with worrisome features should undergo close surveillance imaging. Current consensus guidelines identify high-risk stigmata for malignancy as obstruction jaundice in a patient with a cystic lesion of the head of the pancreas, an enhancing mural nodule ≥5 mm or a solid component, and/or main pancreatic duct dilation ≥10 mm. The presence of these features is associated with an increased risk of high-grade dysplasia or invasive carcinoma and generally warrants consideration for surgical resection in medically fit patients. Our patient presented with obstructive jaundice and marked ventral pancreatic duct dilation to 1.8 cm, both features that prompted surgical resection. The patient had no prior surveillance imaging and no family history of pancreatic cancer.
Despite the presence of pancreas divisum, the surgical approach to an IPMN involving the uncinate process/head does not differ from standard oncologic principles. Achieving negative resection margins is critical in IPMN management, as the presence of dysplasia at the surgical margins is associated with an increased risk of recurrence and may warrant consideration of total pancreatectomy.
In conclusion, ventral duct IPMN in the setting of pancreas divisum is an exceptionally rare entity, with limited cases reported worldwide. This case represents the first documented presentation with obstructive jaundice and the first to lead to malignant transformation in the USA. This case reinforces the importance of high-risk stigmata for IPMN should prompt timely surgical intervention even in patients with pancreas divisum. Increased awareness of this rare association may facilitate earlier diagnosis, prompt timely surveillance, appropriate operative intervention, and improved outcomes.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}