





Abstract
A small bowel perforation caused by ingestion of plant stems or herbal twigs is rare, with inherent diagnostic challenges (i.e. secondary to radiological translucency and nonspecific manifestations). This is a 50 years-old male, who is edentulous and habitually drinks tea using Ocimum every evening, presented to the emergency department with lower-quadrants abdominal pain for 1 day with no prior history of an animal meat-based meal (e.g. fish, chicken). The labs revealed minimal leucocytosis, and the abdominal computed tomography showed a hyperdense linear foreign body penetrating through the terminal ileum. The patient was stable and underwent bowel resection and anastomosis with an uneventful post-operative course. Therefore, even in edentulous patients with no foreign bodies (e.g. bones, toothpicks) possibly ingested, herbs might be a rare cause worthy of investigation.
Introduction
Rarely, a plant-based foreign body ingestion lead to alimentary complications (e.g. perforation) which is an under-recognized clinical phenomenon depending on local culinary practices. The non-specific manifestations (e.g. abdominal pain), an equivocal abdominal examination (e.g. abdominal tenderness) and labs (e.g. insignificantly elevated inflammatory markers) with an unclear radiological outcome (e.g. a translucent object on X-ray) cause a diagnostic conundrum during consultations. This case showed the importance of multidisciplinary collaboration and observation for optimal surgical care [1].
Case presentation
This is a 50 years-old, medically and surgically free male who presented to the emergency department with a one-day history of lower abdominal pain, awakening him from sleep with no other gastrointestinal, constitutional, urinary or respiratory manifestations. In addition, the patient denied ingestion of solid foods (e.g. fish, chicken) or oral instrumentation (e.g. use of dentures or toothpicks). The vital signs were unremarkable, noted edentulous and the pain subsided significantly (was 9/10 in severity and currently 5) after fluids and paracetamol, however upon abdominal examination the patient had lower-quadrants tenderness and rebound tenderness. The laboratory investigations showcased an elevated white blood cells count of 14 (normal range of 4–10) only, with unremarkable other inflammatory markers and tests (e.g. liver and renal functions). The erect chest and abdominal X-rays were unremarkable, however his abdominal computed tomography (A-CT) showed multiple hyperdense, intra-luminal, small bowel foreign bodies with a suspicious linear hyperdense object in the terminal ileum (Fig. 1a and b).
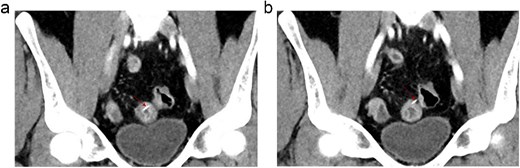
(a, b) Selected coronal images of A-CT post contrast show a dense linear foreign body (red arrows) within the distal ileal loops with pointed end of the linear structure noted possibly penetrating through the small bowel wall protruding to the peritoneal cavity with associated local bowel wall thickening with submucosal edema and mucosal hyperemia. No evidence of adjacent free fluid or free air. No significant surrounding fat stranding.
Accordingly, after discussion with the radiologists to further evaluate this hyperdense foreign body (Fig. 2), a shared decision with the patient was reached to conservatively observe the patient for 24 hours while keeping him nil per oral, on intravenous fluids, antibiotics and analgesia; noting that if the pain did not subside, surgical exploration is mandatory. After 24 hrs, the patient’s pain improved, passed bowel motion and his abdominal examination showed no tenderness or rebound tenderness, however his C-reactive protein was elevated (70) with unremarkable other labs and serial abdominal x-rays. A follow up A-CT was done to assess the foreign body status (anatomical site) and showed complete small bowel wall penetration and fat-stranding with no other manifestations (e.g. pneumatosis, abscess) (Fig. 3a and b).
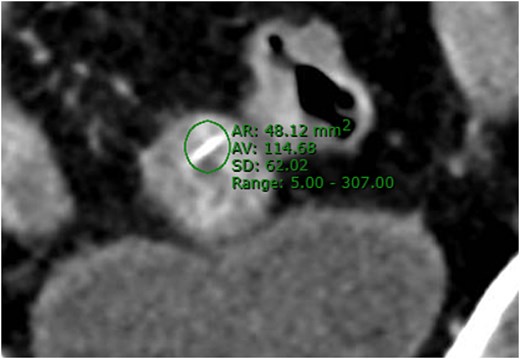
Selected A-CT coronal image showing the linear foreign body with ROI (region of interest) measurement of maximum density of the structure reaching 307 HU and also no streaking artefact is seen. These features indicate that the structure is of moderate density and non-metal material.
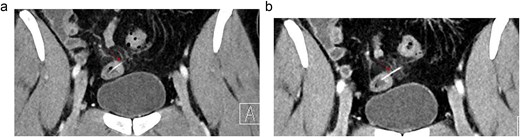
(a, b) Selected coronal images of A-CT with contrast done as follow up after 24 hours showing again the foreign body (arrows) penetrating the bowel wall and partially extending into the mesentery with development of surrounding mesenteric fat strand. No free air or fluid collection.
The patient was informed and prepped for surgical exploration in which intra-operatively a penetrating foreign body was noted ~1 meter from the ileo-caecal valve with bowel wall dusky changes. The decision intra-operatively was to do a small segment resection and anastomosis (Fig. 4a and b). Post-operatively, upon further questioning, the foreign body was identified as a dried Ocimum herb branch used in his daily tea, the patient was doing well throughout and discharged.
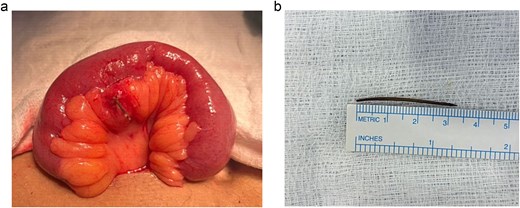
(a, b) Showing the mesenteric border penetration of the terminal ileal segment with abnormal mesentery, and the foreign body retrieved and measured 3 cm.
Discussion
Accidental foreign body ingestion in adults is relatively uncommon; however, elongated organic materials may result in significant gastrointestinal complications (e.g. impalement). The published reports of bowel perforation involve different foreign bodies (e.g. bones, or dentures), whereas perforation caused by ingestion of plant stems or herbal twigs remains rare [2, 3]. These foreign bodies are particularly challenging because they are frequently ingested unnoticed during meals and are often radiolucent on routine imaging [3, 4]. The risk factors reported in the literature include edentulism, rapid eating, impaired mastication, alcohol use, neurological disorders, and decreased oral sensory perception [2, 5]. In addition, several published cases occurred in otherwise healthy individuals without clear predisposing conditions, suggesting that ingestion may remain entirely unrecognized until complications develop [3, 6]. Similar reports involving wooden or plant-derived foreign bodies demonstrated that even relatively small organic fragments may traverse the gastrointestinal tract silently before causing localized sequelae (e.g. abscess formation or perforation) [3, 6].
The anatomical narrowing points (e.g. ileocecal valve, rectosigmoid junction) are the most commonly reported sites of perforation, with delayed diagnosis consistently associated with increased morbidity (e.g. intra-abdominal sepsis) [2–4]. The radiological diagnosis may be challenging, as plant stems and wooden materials are often poorly visualized on plain radiography due to their low radiodensity [4]. Consequently, initial imaging findings may appear nonspecific or falsely reassuring despite ongoing bowel injury. Recent literature emphasizes that CT remains the most useful diagnostic modality because it can identify indirect signs of perforation (e.g. bowel wall thickening, fat stranding) even when the foreign body itself is difficult to visualize [4, 7]. Several published reports noted that definitive diagnosis was ultimately achieved intra-operatively following persistent symptoms or clinical deterioration despite conservative management [3, 6]. Furthermore, management depends on symptom severity, anatomical location, and the presence of complications. Conservative treatment with close observation may be appropriate in clinically stable patients without evidence of obstruction or perforation [7]. However, sharp organic foreign bodies should be considered high risk because of their potential for delayed bowel injury and perforation [2, 3]. Clinical deterioration, persistent pain, peritoneal signs, sepsis, or radiological evidence of perforation generally necessitate urgent surgical intervention [2, 7].
Conclusion
The risk of small bowel perforation caused by ingestion of plant stems is rare, with inherent diagnostic challenges (i.e. secondary to radiological translucency and nonspecific manifestations). Accordingly, elaborate history-taking, vital signs, abdominal examination and laboratory findings with correlation to A-CT findings are key for early detection and follow-up. The awareness of unusual dietary or herbal exposures may facilitate earlier diagnosis and prevent potentially life-threatening complications (e.g. sepsis). Therefore, in edentulous patients with no history of foreign bodies (e.g. toothpicks) ingestion, herbs might be a rare cause worthy of investigation.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}