





Abstract
Cecal volvulus is a rare cause of large bowel obstruction with cecal bascule being a rare cause of cecal volvulus. We present a case of cecal bascule in a 27-year-old female with Kartagener’s syndrome and complete situs inversus with no history of prior abdominal surgeries. Computed tomography imaging revealed complete heterotaxia of the intra-abdominal organs with displacement of the cecum to the left upper quadrant with anteromedial rotation concerning for cecal bascule. The patient was taken urgently to the operating room where an upper midline laparotomy was performed. The cecum was found to be edematous with a distinct area of obstruction consistent with radiographic findings and an ileocecectomy was performed. Recognition of rare diagnoses can be rendered even more difficult in a patient with complete situs inversus and requires a high index of suspicion.
Introduction
Cecal bascule is a rare form of cecal volvulus accounting for ~ 5%–20% of cases [1, 2]. It results from anterior folding of the cecum onto the ascending colon without any torsion [1, 3]. Situs inversus has been associated with intestinal malrotation and volvulus predominantly seen in infants [4]. However, there have been documented case reports of small bowel obstruction in adult patients with situs inversus [4, 5]. Imaging findings of acute intra-abdominal pathologies are rendered more difficult in patients with situs inversus given the altered anatomy [6]. To our knowledge, this is the first documented case of a cecal bascule in an adult patient with complete situs inversus. Written informed consent was obtained from the patient prior to the submission of this manuscript.
Case report
A 27-year-old female with a history of Kartagener’s syndrome with complete situs inversus and prior spinal fusion after a motor vehicle accident presented to the emergency department (ED) with a 1-day history of abdominal pain. The pain was constant and awakened the patient from sleep. Upon presentation to the ED, the patient was hemodynamically stable with no leukocytosis. Her abdominal pain was predominantly located in the left upper quadrant. Computed tomography (CT) imaging was obtained which revealed complete situs inversus with anteromedial rotation and dilation of the cecum concerning for cecal bascule (Fig. 1). The patient underwent prior CT imaging with the cecum located in the left lower quadrant (Fig. 2). A surgical consultation was obtained and the patient was taken to the operating room where an exploratory laparotomy was performed. Intraoperative findings were significant for an edematous cecum with an area of obstruction consistent with the radiographic findings and the diagnosis of cecal bascule. The decision was made to proceed with surgical resection to prevent recurrence. An ileocecectomy was performed with creation of a primary, side-to-side stapled ileocolic anastomosis. The patient’s postoperative course was complicated by delayed return of bowel function as well as a pelvic fluid collection which was aspirated but did not have any bacterial growth. Review of the specimen by pathology revealed the ileocecal valve with mucosal ischemic changes as well as cecal congestion and edema consistent with the diagnosis of cecal bascule.
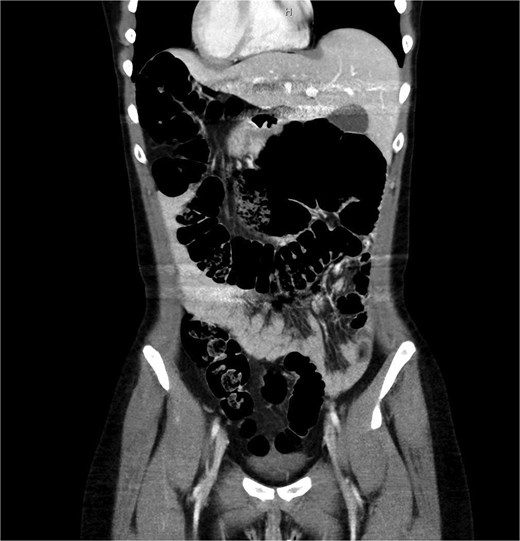
Cecal bascule in patient with situs inversus.

Normal cecal orientation in patient with situs inversus.
Discussion
Cecal bascule is an infrequent cause of cecal volvulus which is due to hypermobility of the cecum resulting in anterior displacement of the cecum without torsion [1, 3, 7]. This creates a functional closed loop obstruction in patients with a competent ileocecal valve which can result in distention, ischemia, and perforation of the cecum [7, 8]. The vast majority of reported surgical strategies for the management of cecal bascules include surgical resection with a right hemicolectomy and creation of a primary ileocolic anastomosis [8, 9]. Situs inversus as seen in patients with Kartagener’s syndrome can make an already challenging diagnosis even more so in the case of cecal bascule as seen in our patient who presented with left upper quadrant abdominal pain. In patients where the diagnosis of situs inversus is unknown this can result in a delay in the diagnosis and treatment of acute intra-abdominal pathologies [10]. A high index of suspicion and early imaging are imperative for the diagnosis and management of intra-abdominal pathology in this rare patient population. To our knowledge, this is the first documented case of a cecal bascule in an adult patient with complete situs inversus.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}