





Abstract
Persistent descending mesocolon (PDM) is a congenital failure of fusion of the descending mesocolon, resulting in a lack of retroperitoneal fixation, rightward displacement, adhesions, and vascular displacement that complicate colorectal surgery. Renal cell carcinoma (RCC) metastasis to the rectum is extremely rare. The patient was a 65-year-old man who had a history of RCC with a rectal tumour. Colonoscopy revealed a submucosal tumor-like lesion, and endoscopic ultrasound-guided fine needle aspiration confirmed metastatic RCC. The shape of the colon on the 3D CT suggested PDM. On operation, adhesions had formed between the transverse and sigmoid colon. First, robot-assisted adhesiolysis was performed, thereby enabling conventional rectal resection. The postoperative course was uneventful. We reported a rare case of rectal metastatic tumor. This case also had PDM, and we needed to perform a non-standard procedure. This report will assist in similar cases of disease in the future.
Introduction
Persistent descending mesocolon (PDM) is an anatomical variation that is a fetal malfusion of the descending colonic mesentery [1, 2], resulting in no fixation to the retroperitoneum and a rightward displacement. PDM may cause adhesions between mesenteries and displacement of blood vessels, complicating the identification of dissection planes and the management of blood vessels during colorectal surgery. According to Minghong et al. [3], PDM can be classified into three types based on the course of the left colon.
On the other hand, RCC is a malignant tumor prone to hematogenous metastasis, yet gastrointestinal metastases occur in <1% of cases [4], with rectal metastases remaining at the level of case reports. Rectal metastases from RCC often do not form lesions on the mucosal surface and present as submucosal tumors (SMTs); therefore, endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) is useful for histological diagnosis [5]. We report a case in which we performed robot-assisted anterior resection following preoperative diagnosis by EUS-FNA for an RCC metastasis arising in the rectum against a background of PDM.
Case presentation
A 65-year-old male who underwent robotic partial nephrectomy for bilateral RCC in 2019. Routine follow-up computed tomography (CT) identified a 20-mm mass in the rectal wall. Colonoscopy showed an SMT-like elevation, and ink marking was performed at the anal side of the tumor. EUS revealed a well-defined, hypoechoic tumour in the submucosa, and FNA was performed. The pathological findings showed cytological features suggestive of clear cell carcinoma as metastatic RCC. Based on this result, we did not perform the positron emission tomography–computed tomography (PET-CT). On imaging, the sigmoid colon was displaced superiorly due to inadequate fixation at the sigmoid-descending colon junction (SDJ), suggesting PDM. The tumor was confined to the left side of the rectum, with no other neoplastic lesions identified within the pelvis (Figs 1 and 2).
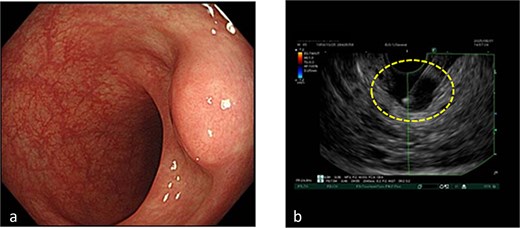
Colonoscopy findings. (a) A tumor suggesting an SMT in the rectum. (b) EUS revealed a cystic lesion (dotted circle) in the rectum, and FNA was performed.
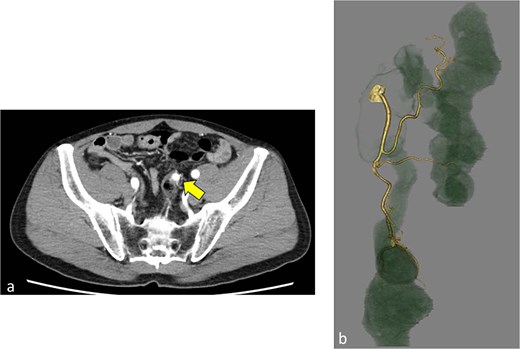
Images of CT. (a) High-density tumor (arrow) in the rectum. (b) 3D image of the colorectum and inferior mesenteric artery.
Anatomical characteristics of PDM
PDM is an anatomical variation where the descending colonic mesentery fails to adhere to the retroperitoneum, leaving the descending colon mobile and intact. The descending colon is displaced to the right and adheres to the mesentery of the small intestine and the mesocolon. Additionally, the sigmoid mesocolon is shortened, and abnormalities such as direct branching from the left colic artery to the rectal artery or an abnormal marginal arterial arch may be observed. Consequently, identifying the dissection plane and managing the vessels can sometimes prove difficult. In the previous report, PDM was classified into three types. Type 1: Isolated rightward displacement of the descending colon, with the sigmoid colon in its normal position. Type 2: Rightward displacement of both the descending colon and the sigmoid colon. The sigmoid colon, which had shifted to the right, was adherent to the right-sided organs. Type 3: The mesentery at the junction of the descending colon and the sigmoid colon was not fixed; as a result, the lower part of the descending colon was inverted upwards, and the sigmoid colon was also displaced upwards. This case is type 3 [3].
Surgical findings
A robot-assisted anterior resection was performed using the da Vinci Xi system. Port placement is shown in the figure (Fig. 3a). The tumour and marking were in the rectum. The transverse colon and sigmoid colon were adherent, and the mesosigmoid was present in a folded manner. To perform adhesiolysis, Targeting was placed at the splenic flexure. The procedure commenced with Port 1 (bipolar), Port 2 (camera), and Port 3 (scissors). After achieving sufficient adhesiolysis, a standard medial approach became feasible. The robot was redocked, Targeting was placed at the SDJ, and a conventional rectal resection was initiated. A medial approach was used to perform a mesenteric incision; however, due to mesenteric torsion, it was difficult to identify the inferior mesenteric artery (IMA) and the left colic artery. Consequently, the vessel was ligated at a site presumed to be the superior rectal artery. Rectal mobilization was performed as standard, followed by en bloc resection of the rectum. Blood flow was confirmed using Indocyanine green, and an anastomosis was performed. Total operative time was 308 minutes (console time: 270 minutes), and blood loss was 2 ml. Intraoperative complication was none (Figs 3–5) (Supplementary video 1).
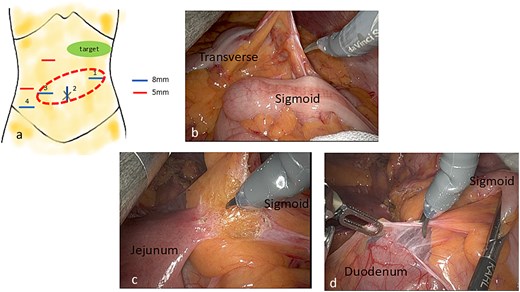
Port site placement and intraoperative findings. (a) The red dotted circle indicates the ports initially used. (b) Adhesions between the sigmoid colon and transverse colon. (c) Adhesions of the jejunum and mesentery of the sigmoid colon. (d) Adhesions of the duodenum and mesentery of the sigmoid colon.
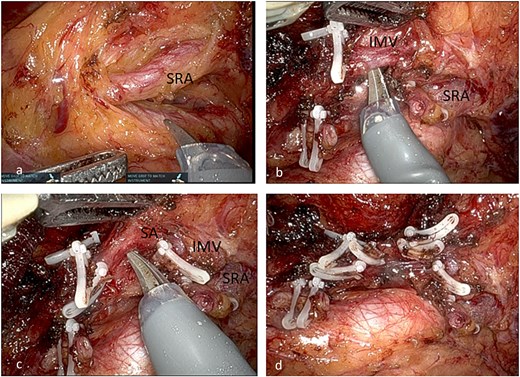
Intraoperative findings of the vessel removal. (a) SRA. (b) IMV. (c) Sigmoid artery (SA). (d) Post vessel ligation.
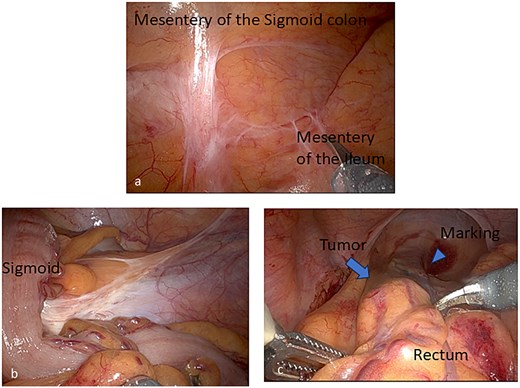
Other intraoperative findings. (a) Adhesions of the ileum and mesentery of the sigmoid colon. (b) Loose adhesion of the SDJ. (c) The tumor elevation (arrow) and marking ink (arrowhead) in the rectum.
The postoperative course was well and no complications. The patient left the hospital on the 6th day after the operation.
Pathological findings
Submucosal tumor measuring 10 × 9 × 7 mm. Diagnosed as clear cell carcinoma with round nuclei and pale cytoplasm extending from the submucosa to the muscularis propria. Immunohistochemistry: PAX8 positive, CD10 positive, CK7 negative. Resection margins negative (R0) (Fig. 6).
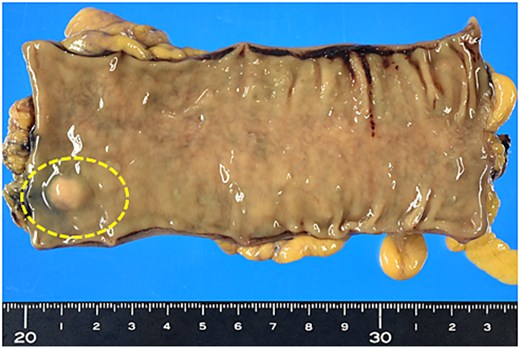
Macroscopic findings of the specimen. SMT-like lesion in the rectum (dotted circle).
Discussion
Rectal metastases from RCC are extremely rare [4], and preoperative diagnosis is difficult [6]. In this case, the key point is the definitive diagnosis of RCC metastasis achieved via EUS-FNA. Furthermore, PDM causes rightward displacement and shortening of the descending colon, adhesions with the mesocolon, and displacement of vascular courses [2]. This makes identification of dissection planes and vascular management more challenging than in standard rectal surgery. Its incidence is approximately 2%. Exposure of the IMA may also prove difficult [1]. The literature classifies this into three types; the present case is diagnosed as type 3, characterized by upward displacement due to SDJ fixation failure [3]. In this type, the transverse and sigmoid colons are adherent, but the IMA rarely courses to the right of the aorta. However, due to the shortened, twisted mesentery or adhesions with other organs, there is a risk of injury to the marginal arterial arch [1, 2, 7]. Patterns where the LCA is deficient are also observed. Consequently, extensive bowel resection may be required due to compromised blood flow.
The literature reports factors such as prolonged operative time, increased blood loss, and higher rates of anastomotic leakage [1, 8, 9]. Compared with robotic surgery, laparoscopy facilitates easier modification of the approach and is well-suited for adhesiolysis at various sites. Conversely, robotic surgery enables delicate adhesiolysis due to its magnified visualization; however, the field of view is typically limited to a local area. In cases like this, where anatomy is significantly displaced, obtaining an overall view may take considerable time. Some reports describe cases in which laparoscopic adhesiolysis was performed to restore near-normal anatomy before proceeding to robotic surgery [1, 7, 10]. However, in PDM, adhesions to the small intestinal mesentery and the right pelvic cavity are often extensive, posing a high risk of damage to surrounding organs during lysis. Furthermore, the dense branching of vessels from the IMA and its abnormal course necessitate particular caution in vascular management [7]. In this case, vascular management also required meticulous ligation and division, differing from standard practice. Moreover, due to the complexity of vascular handling, the risk of injury causing hemodynamic compromise was higher than usual. Consequently, robot-assisted surgery, with its superior precision, is considered suitable for complex adhesiolysis and vascular management, and the objective assessment of residual intestinal blood flow using ICG fluorescence [8] is considered extremely valuable.
There have been no previous reports on robotic-assisted surgery for metastatic rectal cancer; this constitutes the first such report. A particular advantage of robotic surgery is the ability to perform precise maneuvers using multi-jointed forceps. This allows for adaptation to anatomical variations, enabling the safe resection of tumors whilst minimizing blood loss. Furthermore, even in cases involving complex adhesiolysis requiring re-targeting or re-docking, as in this case, the three-dimensional visual field facilitates the identification of fine anatomical layers, enabling adhesiolysis with minimal tissue damage through precise manipulation.
Conclusion
In this rare case of metastatic rectal tumor with PDM, we were able to safely perform a robot-assisted rectal resection following preoperative diagnosis by EUS-FNA. Although anatomical variations associated with PDM increase the difficulty of rectal surgery, robotic surgery proves useful in overcoming these challenges.
Acknowledgements
The authors thank the work of past and present members of our department.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}