





Abstract
Giant inguinoscrotal hernias (GIH) are rare and are often complicated by loss of domain (LOD), incarceration, and chronic soft tissue changes. We report a 51-year-old male with a 30-year history of a progressively enlarging left inguinoscrotal hernia extending to the knee, who presented with abdominal pain and leukocytosis. Computed tomography demonstrated marked LOD without strangulation. Intraoperatively, a large scrotal abscess with soft tissue necrosis was identified in the setting of chronic dense bowel adhesions and spermatic cord involvement. Management required combined abdominal and inguinoscrotal approaches, small bowel resection with anastomosis, orchiectomy, and bilateral anterior component separation with absorbable biosynthetic mesh reinforcement. Due to concern for abdominal compartment syndrome following closure, the patient required planned postoperative intubation and paralysis. He was discharged on postoperative day 9 without major complications. This case highlights the complexity of GIH repair and underscores the importance of individualized operative planning and multidisciplinary perioperative management.
Introduction
Inguinal hernias are among the most common surgical conditions worldwide, with an estimated lifetime risk of 27% in men and 3% in women [1]. Giant inguinoscrotal hernias (GIH) are a rare subtype, typically defined as an inguinal hernia that extends below the midpoint of the inner thigh when standing [2, 3]. They most often arise from prolonged delay in treatment and are encountered infrequently in developed countries, likely reflecting improved healthcare access and earlier elective repair [4].
Unlike routine inguinal hernias, GIHs are frequently associated with loss of domain (LOD), in which a substantial portion of abdominal contents chronically resides outside the abdominal cavity [5]. Reduction of these contents can markedly increase intra-abdominal pressure, leading to respiratory compromise or abdominal compartment syndrome [6, 7]. Surgical management is further complicated by chronic adhesions, bowel fixation, and soft tissue changes, including infection or abscess formation [8, 9]. No standardized operative approach exists for GIH with LOD, and management is guided by safe visceral reduction and durable fascial repair.
Case description
A 51-year-old male with a body mass index of 24.09 kg/m2, prior appendectomy, daily cigarette use (1/2 pack per day), and no other significant medical comorbidities presented with a chronically enlarging left inguinoscrotal hernia of approximately 30 years’ duration. He had been asymptomatic until several days prior to presentation, when he developed abdominal pain radiating to the left scrotum and one episode of non-bloody, non-bilious emesis. Examination revealed a large, irreducible hernia extending to the level of the knee with scrotal skin induration and thickening (Fig. 1). The abdomen was soft without signs of peritonitis.

Preoperative clinical photograph demonstrating a giant left inguinoscrotal hernia extending to the level of the knee in the supine position.
Laboratory studies demonstrated leukocytosis and anemia. Computed tomography of the abdomen and pelvis demonstrated a massive left inguinal hernia with marked LOD containing multiple loops of small bowel and mesenteric fat, without evidence of obstruction or strangulation (Fig. 2).
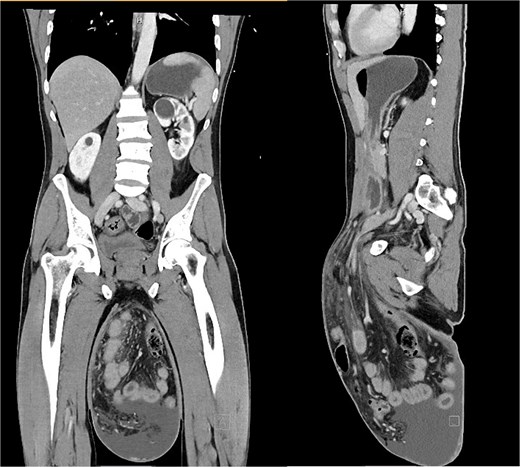
Computed tomography of the abdomen and pelvis with intravenous contrast (coronal and sagittal views) demonstrating a large left inguinoscrotal hernia containing small bowel and colon with loss of domain, without evidence of obstruction or strangulation.
Given the size and chronicity of the hernia, open repair via midline laparotomy was planned with anticipated component separation. The patient was classified as American Society of Anesthesiologists (ASA) Physical Status II. Preoperative cefazolin was administered, and intraoperative ceftriaxone and metronidazole were initiated. At laparotomy, dense adhesions prevented intra-abdominal reduction. An oblique inguinoscrotal incision was performed, revealing a large abscess cavity with necrosis of scrotal soft tissue and omentum. The bowel was congested but not ischemic. During adhesiolysis, an enterotomy occurred, necessitating resection of a friable segment of distal small bowel densely adherent to the abscess cavity. A stapled side-to-side functional end-to-end anastomosis was then performed. The hernia sac and necrotic scrotal tissue were excised, and orchiectomy was required due to involvement of the spermatic cord.
The remaining herniated contents were successfully reduced into the abdominal cavity and a Cooper’s ligament repair was performed. Due to marked LOD, bilateral anterior component separation was performed to facilitate fascial closure. The external oblique aponeuroses were released bilaterally, allowing midline fascial closure with running looped PDS sutures. Peak airway pressures increased from 15 to 26 cm H₂O during closure, raising concern for abdominal compartment syndrome and prompting planned postoperative intubation and paralysis. An onlay absorbable biosynthetic mesh (GORE® ENFORM Biomaterial) was placed for reinforcement given the contaminated operative field. Scrotoplasty was performed with excision of redundant scrotal skin. Two scrotal drains and four abdominal Jackson-Pratt drains were placed.
Postoperatively, the patient remained intubated and paralyzed overnight with bladder pressure monitoring. Paralytics were discontinued on postoperative day 1 and intravenous ceftriaxone and metronidazole were continued until postoperative day 4. The Foley catheter and right scrotal drain were removed by postoperative day 7, and he transitioned from total parenteral nutrition to an oral diet by postoperative day 9. He was discharged home on postoperative day 9 in stable condition with abdominal and left scrotal drains in place (Fig. 3). At 3-week follow-up, he reported improving bowel function, full ambulation, and well-healed incisions without evidence of seroma, hematoma, or infection. At 4-month follow-up, the patient remained asymptomatic with no evidence of recurrence (Fig. 4).

Postoperative day 9 clinical photograph demonstrating closed midline abdominal incision with sutures and staples, 2 abdominal drains, and 1 scrotal drain following hernia repair and reconstruction.

Clinical photograph at 4-month follow-up demonstrating well-healed abdominal and scrotal incisions with restoration of abdominal wall and scrotal contour.
Final pathology demonstrated a 48-cm segment of small bowel with serosal adhesions, granulation tissue, and necrotic mesenteric fat without malignancy (0/3 lymph nodes). The scrotal specimen showed chronic inflammation and necrosis of peri-testicular soft tissue, benign scrotal skin with mixed acute and chronic inflammation, and a testis with reduced spermatogenesis without germ cell neoplasia.
Discussion
GIHs develop over years of progressive enlargement, resulting in anatomical distortion and physiologic adaptation. A key challenge is LOD, in which abdominal viscera reside chronically outside the abdominal cavity. Reduction may therefore increase intra-abdominal pressure, risking respiratory compromise and abdominal compartment syndrome [5]. No standardized operative guidelines exist, but various strategies have been described, including staged repair, component separation techniques, and use of traction to expand the abdominal cavity [3, 10, 11].
Severe complications such as bowel necrosis and advanced soft tissue changes may necessitate additional operative interventions. Scrotal abscesses may develop secondary to chronic ischemia, skin breakdown, or bowel perforation [12]. Even non-ischemic bowel may require resection in the setting of dense adhesions or chronic inflammation preventing safe reduction. Chronic enlargement may also necessitate reconstructive procedures such as scrotoplasty or penile reconstruction [13, 14].
Management of GIH with LOD often requires multidisciplinary planning involving surgery, anesthesia, and critical care teams due to the risk of abdominal compartment syndrome and prolonged postoperative ventilation. Preoperative counseling should address the physiologic consequences of abdominal closure and the possibility that definitive repair may not be feasible. Adjunctive tools such as P-POSSUM or CeDAR may further assist perioperative risk assessment in complex abdominal wall reconstruction.
This case highlights the importance of individualized operative planning and multidisciplinary management in GIH complicated by LOD, infection, and dense adhesions. Chronicity may necessitate adjunctive procedures such as bowel resection, orchiectomy, and advanced abdominal wall reconstruction. Early evaluation and elective repair remain critical to prevent complications associated with long-standing disease.
Conflicts of interest
None declared.
Funding
None declared.
Consent statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}