





Abstract
Adult intussusception is rare, accounting for ~1% of intestinal obstruction cases, and most cases are caused by neoplastic lesions. This report describes a 30-year-old male patient with a solitary Peutz–Jeghers syndrome hamartomatous polyp that mimicked colon cancer preoperatively. The patient had no mucocutaneous pigmentation, family history of polyposis or malignancy, and no STK11/LKB1 mutation. Whole-exome sequencing identified two novel heterozygous variants in POLE and EXO1. Intraoperative exploration of the terminal ileum is critical to avoid misdiagnosis and unnecessary colectomy.
Introduction
Adult intussusception is rare, occurring in ~1% of cases with bowel obstructions [1]. Neoplasms are the predominant etiology in adult, primary colonic malignancies account for two-thirds of adult intussusception, while benign tumors, such as adenomatous polyps and lipomas contribute to 25% of cases [2]. Peutz–Jeghers syndrome (PJS)-associated hamartomatous polyp is a rare autosomal dominant disorder characterized by gastrointestinal polyposis, mucocutaneous pigmentation, and family predisposition [3]. The histopathological feature of a typical PJS hamartomatous polyp exhibit a branched, frond-like architecture with a stromal core containing smooth muscle, and surrounded by near-normal epithelium [4]. Solitary PJS polyps typically lack phenotypic features and family history, leading to substantial diagnostic difficulty. Here, we present a rare case of solitary intestinal PJS polyp causing adult intussusception and mimicking colonic carcinoma.
Case report
A 30-year-old male presented with chronic intermittent abdominal pain and nausea persisting for 1 year. Physical examination revealed no mucocutaneous pigmentation. Family history was negative for gastrointestinal polyposis or malignancies. Routine laboratory examinations were unremarkable. Abdominal computed tomography (CT) demonstrated a target sign indicative of intussusception (Fig. 1a–c). Preoperative colonoscopy showed a large neoplastic lesion in the ascending colon, and biopsy indicated a benign polypoid lesion. The preoperative diagnosis was intussusception secondary to an ascending colon tumor (Fig. 1d).
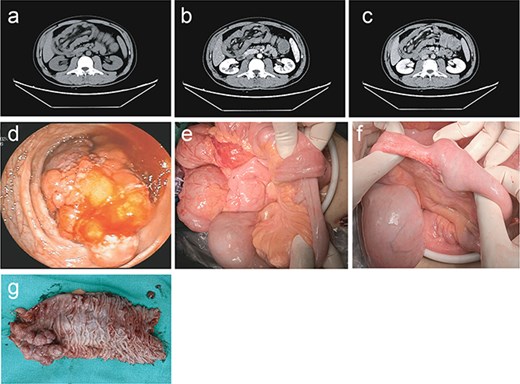
Preoperative, intraoperative, and postoperative findings. (a) Abdominal non-contrast CT indicated “target sign,” which can be shown from intussusception, was identified in the terminal ileum. (b) Enhanced CT in arterial phase revealed uniform enhancement of intestinal wall within intussusception, no significant enhancement of mass observed. (c) Enhanced CT in venous phase revealed a persistent “double duct sign.” (d) Preoperative colonoscopy examination identified a large solitary lobular polyp with proliferating glandular tissue and muscular core. (e) Intraoperative finding indicated the terminal ileum intussusception. (f) Intraoperative finding indicated a firm mass was palpable within the terminal ileum. (g) Postoperative gross specimen indicated a cauliflower-like mass growth which has not penetrated the serosa.
Laparoscopic exploration of the entire colon detected no mass. Intraoperative colonoscopy via the ileocecal valve also revealed no colonic polyps or tumors. Repeated laparoscopic exploration identified a mass in the terminal ileum (Fig. 1e and f). Segmental intestinal resection and anastomosis were performed smoothly, and the patient had an uneventful postoperative recovery. Postoperative histopathology confirmed a solitary PJS hamartomatous polyp (3 × 3 cm, pedunculated, well-circumscribed) (Fig. 1g). Hematoxylin and eosin staining showed arborizing smooth muscle bundles derived from the muscularis mucosae and superficial foveolar epithelial hyperplasia, consistent with PJS features (Fig. 2a–d).
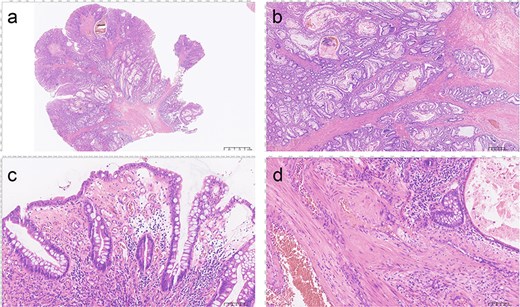
Histopathologic findings (hematoxylin and eosin staining). (a) Hematoxylin and eosin staining of the resected polyp showing arborizing smooth muscle bundles with overgrowth of superficial foveolar epithelium (2.5 mm). (b) Demonstrating the arborizing pattern of smooth-muscle proliferation, and these smooth muscle bundles were originated from the muscularis mucosa (400 μm). (c) A relatively large amount of lymphocyte infiltration on the surface edematous area (100 μm). (d) A large-scale infiltration of eosinophils in the stroma (100 μm).
Whole-exome sequencing showed no STK11/LKB1 mutation but identified two novel heterozygous variants: POLE c.1202A>G (p.Q401R) and EXO1 c.295A>C (p.N99H). At 1-year follow-up,
gastroscopy and enteroscopy showed no other space-occupying lesions.
Discussion
This patient presented with chronic incomplete intestinal obstruction due to intussusception and was misdiagnosed with ascending colon cancer preoperatively. The absence of mucocutaneous pigmentation and family history further complicated diagnosis. Patients with PJS carry a high cumulative risk of intussusception, usually induced by small-bowel hamartomas ≥15 mm in diameter [5]. Polyps in the terminal ileum may show pseudoinvasion, which can be easily misdiagnosed as invasive carcinoma [6].
Solitary PJS polyp is extremely rare; it shares identical pathological features with classic PJS but lacks typical phenotypic, familial, and STK11 mutation characteristics [4, 6]. Most reported cases are sporadic and located in the stomach, duodenum, small intestine, appendix, or colon [7–9]. Solitary small-bowel PJS polyps are even rarer, a MEDLINE search of the well-documented English language literature up to 2026 using the terms “solitary Peutz–Jeghers” and “jejunum,” “ileum” revealed 14 patients with a solitary PJ-type polyp in the jejunum or ileum with a median diagnostic age of 47 years and a size range of 15–72 mm [10] (Table 1).
Cases of solitary jejunum and ileum Peutz–Jeghers polyp, as reported in the literature.
| Case | Year of diagnosis | Author | Age (year) | Gender | Location | Size (cm) | Classic features | STK11 mutation | PMID |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2000 | Sone Y et al. | 64 | Female | Jejunum | 3.0 | Non | Np | 10 805 860 |
| 2 | 2004 | Lantz H et al. | 20 | Male | Jejunum | 1.5 | Non | Np | 15 278 073 |
| 3 | 2013 | Okada H et al. | 22 | Female | Ileum | 3.9 | Non | Np | 23 530 564 |
| 4 | 2018 | Kalliakmanis V et al. | 16 | Female | Jejunum | Np | Non | Non | 29 484 932 |
| 5 | 2019 | Chang H et al. | 55 | Male | Ileum | 4.0 | Non | Np | 29 474 969 |
| 6 | 2020 | Endo K et al. | 29 | Male | Jejunum | 3.0 | Non | Np | 32 779 147 |
| 7 | 2021 | Zhao X et al. | 24 | Male | Jejunum | 1.7 | Non | Np | 33 190 941 |
| 8 | 2022 | Onuma K et al. | 53 | Male | Jejunum | 3.0 | Non | Np | 35 777 377 |
| 9 | 2022 | Aytin YE et al. | 28 | Female | Jejunum | 5.0 | Yes | Yes | 35 652 870 |
| 10 | 2022 | Liu BL et al. | 43 | Male | Jejunum | 7.0 | Non | Non | 34 955 063 |
| 11 | 2023 | Edmondson E et al. | 33 | Male | Jejunum | 3.0 | Non | Np | 37 206 505 |
| 12 | 2023 | Alenezi T et al. | 81 | Male | Jejunum | 4.0 | Non | Non | 38 146 326 |
| 13 | 2023 | Kamath B et al. | 12 | Female | Jejunum | Np | Non | Non | 37 389 396 |
| 14 | Present case | Liu Z et al. | 30 | Male | Ileum | 3.0 | Non | Non |
Most cases are STK11-negative, supporting that solitary PJS represents a distinct clinical entity separate from classic PJS [11]. Germline POLE mutations predispose individuals to colorectal adenomas and carcinoma [12]. EXO1 variants are associated with attenuated familial adenomatous polyposis and genomic instability [13]. According to ACMG guidelines, POLE p.Q401R is likely pathogenic, while EXO1 p.N99H is a variant of uncertain significance [14]. These findings suggest genetic heterogeneity in solitary PJS.
In adult intussusception, intraoperative colonoscopy and careful exploration of the terminal ileum are essential to avoid misdiagnosis and unnecessary right hemicolectomy. Solitary PJS polyps have low malignant potential and do not require intensive long-term surveillance as in classic PJS [15].
Conclusion
Solitary PJS polyp of the terminal ileum is a rare cause of adult intussusception and can mimic colon cancer preoperatively. Intraoperative exploration of the terminal ileum helps prevent misdiagnosis and unnecessary colectomy. Genetic testing identifies POLE/EXO1 variants, indicating genetic heterogeneity beyond STK11 in this condition.
Author contributions
Hou P. and Liu Z. contributed to conceptualization, formal analysis, data curation, investigation, and writing—original draft. Peng Q., Wen Y.M., Xu G.F., Liu Y.H., and Luo J. contributed to conceptualization, writing—review and editing, and project administration. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
This work was supported by the Jiangxi Natural Science Foundation (Grant No. 20232BAB206102).
Ethics approval and consent
This study was approved by the Ethics Committee of the First Affiliated Hospital of Gannan Medical University. Written informed consent was obtained from the patient for publication of this case report.

{kind=link}
{kind=link}