





Abstract
Uterine angiomyolipomas (AMLs) are exceptionally rare benign mesenchymal tumors that can closely mimic malignant uterine or retroperitoneal neoplasms when large or highly vascular. We describe the case of a healthy 29-year-old postpartum woman who presented with acute abdominal pain three months after delivery and was found to have a rapidly enlarging 10-cm hypervascular mass arising from the right uterine cornua with extension into the retroperitoneum. The imaging appearance and interval growth were highly concerning for a retroperitoneal sarcoma. She underwent diagnostic laparoscopy, which was converted to open resection with multidisciplinary assistance due to deep retroperitoneal involvement. Frozen section was nondiagnostic, prompting total abdominal hysterectomy. Final pathology demonstrated a benign AML composed of smooth muscle, blood vessels, and adipose tissue. The patient recovered uneventfully. This case highlights a rare benign entity that can convincingly simulate sarcoma both clinically and radiographically, emphasizing the diagnostic and surgical challenges when malignancy cannot be excluded.
Introduction
Angiomyolipomas (AMLs) are benign mesenchymal tumors composed of varying proportions of smooth muscle, dysmorphic blood vessels, and adipose tissue [1]. They represent the most common benign renal neoplasm and are frequently associated with tuberous sclerosis complex [2]. Extrarenal AMLs, however, are rare, and occurrence within the uterus is uncommon, with only a small number of cases described in the literature [3].
Uterine AMLs may radiographically resemble leiomyomas, lipoleio-myomas, or high-grade sarcomas depending on their relative tissue composition [4]. Features, such as marked hypervascularity, rapid growth, and retroperitoneal extension, as seen in this case, can heighten suspicions for malignancy. Distinguishing benign from malignant uterine masses preoperatively can be challenging, and definitive management often requires surgical excision.
We present a rare case of a uterine AML with extensive retroperitoneal growth in a young postpartum woman. The mass demonstrated rapid interval enlargement and highly vascular features, raising strong concern for leiomyosarcoma. This case emphasizes the importance of a multidisciplinary surgical approach and the role of pathology in establishing a definitive diagnosis.
Case presentation
A 29-year-old previously healthy woman, three months postpartum following an uncomplicated spontaneous vaginal delivery at 38 weeks and 5 days, presented to the emergency department with several days of progressively worsening abdominal pain. All prenatal and immediate postpartum ultrasounds were normal except for a small right ovarian cyst measuring ~3 cm. A CT scan obtained in the emergency department demonstrated a heterogeneous right adnexal mass measuring ~9.2 × 4 × 7 cm, initially believed to arise from the ovary. She was discharged with analgesics and referred to her obstetrician–gynecologist for further evaluation.
At her outpatient follow-up, laboratory testing revealed an elevated inhibin B level of 275 pg/ml, while CA-125, CA 19-9, carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), and lactate dehydrogenase (LDH) were within normal limits. A pelvic magnetic resonance imaging (MRI) showed a large, heterogeneous, intensely enhancing, and highly vascular mass arising from the right uterine cornua (Figs 1 and 2). The lesion measured 6.5 × 7.7 × 10.2 cm and demonstrated marked feeding vessels within the adjacent myometrium. The mass displaced the right ovary superiorly but did not appear to originate from it. It extended into the right perirectal retroperitoneal space and abutted the sacrum, displacing but not invading the rectum. No lymphadenopathy or metastatic disease was identified on MRI and review of previous CT imaging. Given its hypervascularity, retroperitoneal extension, and rapid interval growth since the normal ultrasound three months prior, the differential diagnosis being considered included leiomyosarcoma, carcinosarcoma, and other uterine sarcomas. An endometrial biopsy was also performed and was negative for atypia or malignancy, though this was considered low yield because the lesion appeared to originate from the myometrium rather than the endometrium.
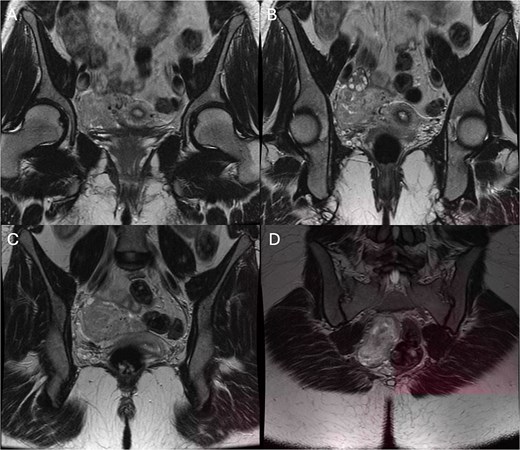
Coronal T2-weighted pelvic MRI images demonstrating a uterine mass with mixed vascular, smooth muscle, and adipose tissue components consistent with AML. Panels (A–D) represent sequential coronal slices.
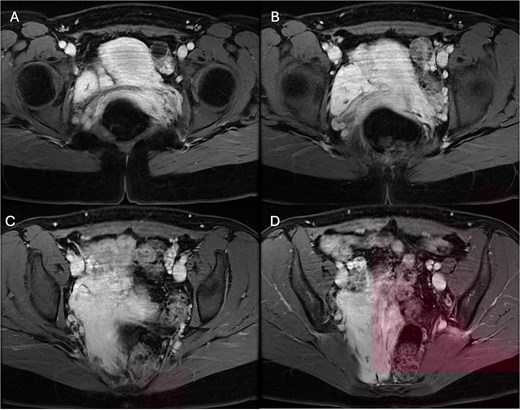
Axial post-contrast fat-suppressed T1-weighted pelvic MRI images (water-only LAVA sequence) demonstrating uterine mass with mixed vascular, smooth muscle and adipose tissue components consistent with AML. Panels (A–D) represent sequential axial slices.
The patient was referred to Surgical Oncology for evaluation of the retroperitoneal component, and the surgical resection was recommended due to the mass’s size, vascularity, and uncertain malignant potential. She had completed childbearing and consented to hysterectomy if frozen section could not definitively exclude malignancy. She subsequently underwent diagnostic laparoscopy, which demonstrated a large retroperitoneal mass which appeared to arise from the right side of the uterus, with normal-appearing ovaries and no peritoneal disease. Due to the deep location and size of the tumor, the operation was converted to an open midline laparotomy. The retroperitoneal mass was carefully dissected circumferentially with Surgical Oncology assistance, with ligation of multiple feeding vessels and preservation of surrounding structures, including the rectum and ureters. The mass was resected en-bloc with its uterine attachment and sent for frozen section.
Frozen section analysis suggested a spindle cell lesion favoring a benign smooth-muscle proliferation but was nondiagnostic and could not exclude sarcoma. Given the patient’s reproductive plans and the inability to determine malignancy intraoperatively, a total abdominal hysterectomy with bilateral salpingectomy was performed, preserving both ovaries, which appeared normal. The postoperative course was uncomplicated, and she was discharged home on postoperative day 2.
Final pathology revealed a benign AML composed of smooth muscle, thick-walled vessels, and mature adipose tissue without atypia or mitotic activity. Immunohistochemistry was positive for desmin and smooth muscle actin (SMA), negative for human melanoma black-45 (HMB-45) and melanoma antigen-A (Melan-A), and cluster of differentiation 34 (CD34) highlighted the vascular component. Kirsten rat sarcoma viral oncogene homolog (KRAS) and KIT proto-oncogene, receptor tyrosine kinase (KIT) mutation analyses were not performed. At postoperative follow-up, the patient was recovering well with no need for additional treatment.
Discussion
Angiomyolipomas are benign mesenchymal tumors composed of smooth muscle, blood vessels, and adipose tissue, most commonly arising in the kidney. Extrarenal AMLs are rare, and uterine involvement is exceedingly uncommon, with only a few isolated case reports in the literature, a selection of which are summarized in Table 1 [3, 5–10]. When they occur in the uterus, their imaging appearance can be highly variable depending on the relative proportions of fat, muscle, and vascular structures. This variability contributes to diagnostic difficulty, particularly when the lesion is large or hypervascular.
Review of published cases of uterine angiomyolipoma, including imaging findings, surgical management, histopathology, and immunohistochemical characteristics.
| Author | Year | Age (yrs.) | Imaging | Size on imaging | Biopsy | Surgical management | Final pathology | Immunohistochemistry |
|---|---|---|---|---|---|---|---|---|
| Laffargue et al. [5] | 1993 | 20 | US, CT | 15 cm | No | Cyst aspiration; Open total hysterectomy with pelvic lymph node dissection | Multilobulated, thinly walled; made of mature adipose tissue (30%), smooth muscle tissue (50%), mature blood vessels (20%) --> uterine angiomyolipoma | (+) desmin (+) vimentin |
| Yaegashi et al. [6] | 2001 | 40 | US, CT, MRI | 12 cm | No | Hysterectomy with right salpingo-oophorectomy | 10 x 8 x 4 cm; composed of numerous blood vessels, smooth muscles, and mature adipose tissue | (+) SMA (+) desmin (+) vimentin (+) anti-human muscle actin (+) PR (−) cytokeratin (−) HMB-45 (−) CD34 (−) S100 (−) ER |
| Yaegashi et al. [6] | 2019 | 43 | US | – | No | Mass excision | Benign unencapsulated lesion with triphasic morphology, suggestive of angiomyolipoma-cervix | (−) HMB-45 |
| Roy et al. [8] | 2022 | 49 | US, CT | 11.3 x 7.5 cm | No | Laparoscopic hysterectomy | 6 x 4 x 3 cm angiomyolipoma of the uterus spindle cells at periphery, abundant myxoid stroma separated by smooth muscle bundles with focal epithelioid morphology; intervening adipocytes and numerous blood vessels | - |
| Verocq et al. [9] | 2022 | 58 | US, MRI, PET | 5.2 x 4.1 x 3.8 cm | No | Total hysterectomy with bilateral adnexectomy and peritoneal cytology | 4 x 3 x 3 cm angiomyolipoma; proliferation of smooth muscle tissue, adipose tissue, and blood vessels; no necrosis | Cytoplasm: (+) desmin (+) clone D33 (+) caldesmon Smooth muscle: (+) focally membranous CD10 All: (−) HMB-45 |
| Kiran et al. [3] | 2023 | 44 | CT | – | Yes | Laparoscopic TAHBSO | 4 x 3 x 2 cm smooth muscle proliferation with prominent blood vessels, patchy hyalinization, scant mature adipose tissue between smooth muscle bundles | (−) HMB-45 |
| Song et al. [10] | 2025 | 49 | US, CT, MRI | 6.23 x 6.38 cm | No | Laparoscopic TAHBSO | Triphasic tumor composed of pleomorphic epithelioid cells (70%), mature adipose cells (20%), and thick-walled, tortuous blood vessels | (+) SMA (−) HMB-45 (−) melan-A (−) S100 in tumor cells (+) S100 in adipose cells (+) CD31 in vascular endothelial cells |
Abbreviations: US, ultrasound; CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography; SMA, smooth muscle actin; PR, progesterone receptor; ER, estrogen receptor; HMB-45, human melanoma black 45; CD34, cluster of differentiation 34; CD31, cluster of differentiation 31; S100, S100 protein; TAHBSO, total abdominal hysterectomy with bilateral salpingooophorectomy.
The presentation in this case was unusual in several respects. The patient had completely normal prenatal and postpartum imaging only months before her diagnosis, followed by rapid interval enlargement to a 10-cm mass with retroperitoneal extension. Postpartum hormonal shifts may contribute to tumor growth in some mesenchymal neoplasms, although this association has not been well defined for AML [11]. The mass demonstrated striking vascularity and displacement of adjacent structures, radiologically mimicking a leiomyosarcoma or other uterine sarcoma. Although AMLs typically contain macroscopic fat, the absence of visible fat on MRI, combined with hyperenhancement and infiltrative-appearing growth, made preoperative diagnosis challenging. The elevated inhibin B further increased concern, as it is widely recognized as a tumor marker for granulosa cell tumors and may also be elevated in other malignant ovarian neoplasms, although it ultimately proved nonspecific in this setting [12].
Management of large or radiologically concerning uterine masses requires careful balancing of diagnostic certainty and surgical risk. Preoperative biopsy was avoided due to the risk of bleeding from a highly vascular lesion and the potential for tumor seeding should the mass have been malignant [13]. Frozen section provided limited reassurance, as spindle cell lesions may overlap morphologically with leiomyosarcoma, and definitive distinction often requires full histopathologic analysis with immunohistochemistry. Given the patient’s complete childbearing and the inability to exclude malignancy intraoperatively, proceeding with total abdominal hysterectomy was appropriate.
This case also underscores the importance of a multidisciplinary approach. The mass extended deeply into the retroperitoneum, abutted the sacrum, and displaced the rectum, features unusual for benign uterine tumors. Collaboration with surgical oncology facilitated safe dissection around critical retroperitoneal structures, allowing for complete en-bloc removal without bowel injury or ureteral compromise.
Final pathology confirmed AML with classic smooth muscle, vessel, and adipose components. The tumor’s immunoprofile (desmin and SMA positive; HMB-45 and Melan-A negative) helped to distinguish it from perivascular epithelioid cell tumors (PEComas) and other entities within the same diagnostic spectrum [14]. Complete surgical excision is generally curative, and recurrence is not expected [8].
Conclusion
This case illustrates a rare presentation of uterine AML with rapid postpartum growth and retroperitoneal extension, radiologically and clinically mimicking uterine sarcoma. The lesion’s unusual vascularity, interval enlargement, and deep anatomic involvement necessitated a multidisciplinary surgical approach and definitive resection to establish diagnosis. Although benign, uterine AMLs may display aggressive features that complicate preoperative evaluation. Awareness of this entity is important when managing large, hypervascular uterine masses, particularly when imaging suggests malignancy and biopsy is not feasible.
Acknowledgements
The authors would like to thank the multidisciplinary surgical and pathology teams involved in the care of this patient.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
This research received no external funding.
Data availability
All data generated or analyzed during this study are included in this published article. Additional details are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
This study was conducted in accordance with institutional ethical standards. Ethical approval was waived as this is a single-patient case report. Written informed consent was obtained from the patient for participation.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

{kind=link}
{kind=link}