





Abstract
Cecal volvulus is a rare cause of acute intestinal obstruction in adults, while intestinal malrotation is typically diagnosed in infancy and only rarely presents in adulthood. We report a rare case of cecal volvulus associated with previously undiagnosed intestinal non-rotation in a 48-year-old patient. The patient presented with acute abdominal pain and was diagnosed with cecal volvulus on computed tomography. Emergency laparotomy confirmed the diagnosis and revealed intestinal non-rotation. The patient was successfully treated with ileocecal resection and primary side-to-side anastomosis. This case highlights the importance of considering congenital rotational anomalies in adult patients presenting with cecal volvulus, as these anatomical variations may predispose to volvulus and may only be recognized intraoperatively.
Introduction
Cecal volvulus is a rare cause of large bowel obstruction in adults, accounting for ~1%–1.5% of all intestinal obstructions [1]. The most common type of colonic volvulus in adults is sigmoid volvulus, for which well-established management strategies exist [2].
Cecal volvulus typically occurs in patients with increased cecal mobility, most commonly due to incomplete peritoneal fixation of the right colon or other predisposing factors such as previous abdominal surgery or chronic constipation [1, 3]. Patients often present with non-specific abdominal pain, typically located in the right lower quadrant, and symptoms may sometimes resolve spontaneously. However, in acute cases it may present as bowel obstruction, and delayed diagnosis can lead to bowel ischemia or perforation [3].
Intestinal malrotation is a congenital anomaly resulting from incomplete rotation and fixation of the midgut during embryological development. It is most diagnosed during infancy, whereas presentation in adulthood is rare and frequently asymptomatic [4, 5]. Non-rotation, a subtype of malrotation, is characterized by right-sided small bowel, left-sided colon, and absence of retroperitoneal fixation of the ascending colon, which increases bowel mobility and may predispose to volvulus [6].
We report a rare case of acute cecal volvulus in a 48-year-old patient, in whom previously undiagnosed intestinal non-rotation was discovered intraoperatively.
Case presentation
A 48-year-old male patient presented to the emergency department with sudden onset of diffuse abdominal pain, progressive abdominal distension, nausea, and vomiting. There was no history of similar episodes in the past. One year earlier, he had undergone an extraperitoneal inguinal hernia repair and umbilical hernia repair in a community hospital; otherwise, he had no history of previous abdominal surgery.
Physical examination revealed a distended and tender abdomen, with pain predominantly in the mid-abdomen, without signs of peritonitis. Laboratory investigations showed a white cell count (WCC) of 15.14 G/L (reference 4–10 G/L), bilirubin of 20.7 μmol/L (<19), and lactate of 2.4 mmol/L (0.5–1.6).
An abdominal ultrasound was initially performed in the emergency department, suggesting possible signs of gastroenteritis. However, due to the patient’s significant abdominal pain, a contrast-enhanced computed tomography (CT) scan was subsequently performed. CT imaging demonstrated a markedly dilated cecum measuring up to 9 cm located in the left upper quadrant, with a whirlpool sign of the mesentery, consistent with cecal volvulus. Additionally, distension of the ileum with a small bowel feces sign was observed, suggesting small bowel obstruction. A small amount of free intra-abdominal fluid was present, but no evidence of bowel ischemia or perforation was identified (Fig. 1).
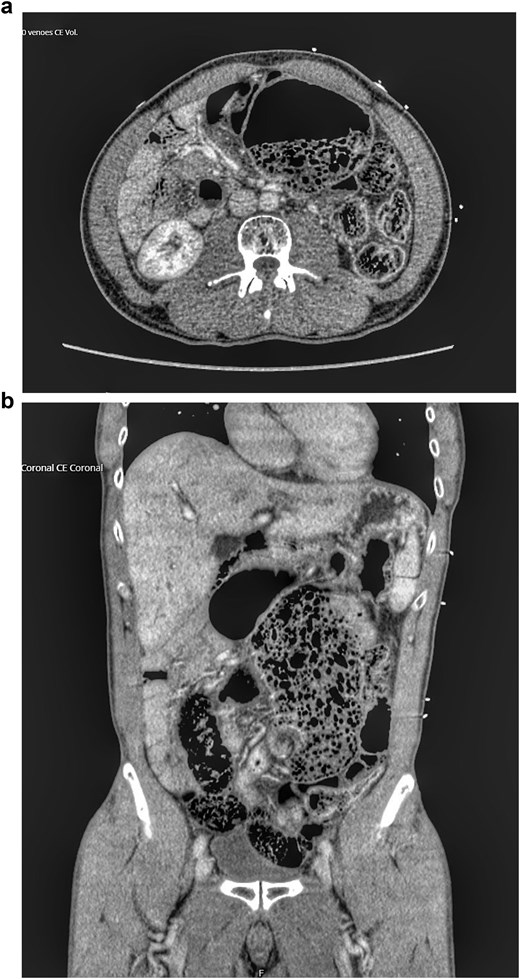
Preoperative contrast-enhanced CT of the abdomen showing cecal volvulus. (a) Axial view demonstrates a markedly dilated cecum. (b) Coronal view shows the twisted cecum and mesentery, consistent with volvulus. No evidence of ischemia or perforation is seen.
A nasogastric tube was inserted in the emergency department. Given the significant cecal distension and the risk of perforation, an emergency laparotomy was performed.
Intraoperatively, a cecal volvulus with markedly dilated and twisted bowel was confirmed, without signs of ischemia. Additionally, it was noted that the small bowel was located predominantly on the right side and the colon on the left side, with absence of retroperitoneal fixation of the ascending colon, findings consistent with intestinal non-rotation (a subtype of malrotation).
An ileocecal resection with primary side-to-side anastomosis was performed, and an intra-abdominal drain was placed. No additional corrective procedure for the malrotation was undertaken.
Postoperatively, the nasogastric tube remained in place due to delayed gastric emptying and was removed 6 days after surgery. The gastroparesis was treated with prokinetic. Following normalization of gastric and bowel function, the nasogastric tube was removed, and gradual diet advancement was well tolerated.
A hypokalaemia occurred during the postoperative course and was treated with electrolyte substitution. The intra-abdominal drain was removed on postoperative day five.
Toward the end of the hospital stay, the patient developed a superficial wound infection. Two skin staples were removed, and the wound subsequently healed by secondary intention. The patient was discharged 10 days after surgery in good clinical condition.
No routine follow-up was scheduled. The patient was seen 2 years later due to a recurrent inguinal hernia and a subjective sensation of an unstable abdominal wall. CT imaging demonstrated bilateral inguinal hernia recurrence and rectus diastasis. As the patient reported only unspecific symptoms, a watch-and-wait approach was adopted.
Discussion
Cecal volvulus in adults is uncommon and generally occurs in the setting of abnormal cecal mobility [1, 7]. Predisposing factors include congenital anomalies, prior abdominal surgery, and chronic constipation. Timely surgical intervention is essential to prevent bowel ischemia or perforation [3].
Intestinal malrotation is usually detected in infancy, whereas adult presentation is rare [4, 8]. Non-rotation, a subtype of malrotation, is characterized by right-sided small bowel and left-sided colon, increasing bowel mobility and predisposing patients to volvulus [6].
In adults, malrotation is often asymptomatic and may remain undetected until incidentally discovered during imaging or surgery for unrelated conditions [4].
In the present case, preoperative CT identified the cecal volvulus but did not initially suggest the underlying intestinal non-rotation, which was recognized only intraoperatively. In retrospect, subtle radiological signs of non-rotation could be identified on CT imaging, particularly the abnormal displacement of the cecum into the left upper quadrant. However, these findings were not recognized during the emergency assessment [9], where the primary aim of imaging interpretation was confirmation of bowel obstruction and exclusion of ischemia.
The present case is noteworthy for several reasons. First, the intestinal non-rotation was not suspected preoperatively and was diagnosed only during surgery. Second, the patient presented at the age of 48 years, illustrating that congenital rotational anomalies may remain clinically silent for decades. Third, CT imaging demonstrated cecal displacement into the left upper quadrant associated with a whirlpool sign and small bowel feces sign, findings consistent with advanced volvulus.
Management of cecal volvulus generally requires surgical treatment. Surgical options include detorsion alone, cecopexy, segmental resection, or right hemicolectomy [3]. In pediatric patients, intestinal malrotation is typically corrected using a Ladd procedure [4]. However, in adults, the necessity of performing a Ladd procedure for incidentally discovered malrotation remains debated.
Several authors suggest that prophylactic correction is not mandatory in asymptomatic adults, particularly when the bowel is viable and the acute pathology has been treated [6]. In the present case, ileocecal resection with primary anastomosis was performed without additional correction of the malrotation, supporting a tailored surgical approach.
Only a limited number of cases describing the association between cecal volvulus and intestinal non-rotation in adults have been reported in the literature, highlighting the rarity of this condition [10].
Conclusion
Cecal volvulus is a rare cause of acute intestinal obstruction in adults and may occasionally be associated with previously undiagnosed congenital rotational anomalies. Intestinal non-rotation in adulthood is often asymptomatic and may only become apparent during surgery performed for other acute abdominal conditions.
This case highlights the importance of considering congenital anatomical variations in adult patients presenting with cecal volvulus, particularly when preoperative imaging does not clearly demonstrate rotational abnormalities.
Prompt surgical intervention remains essential to prevent bowel ischemia and perforation. In patients with viable bowel, ileocecal resection with primary anastomosis represents a safe and effective treatment, while incidental non-rotation discovered in adulthood does not necessarily require additional corrective procedures.
Awareness of this rare association may help surgeons recognize unusual intraoperative findings and guide appropriate surgical management.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}