





Abstract
A 39-year-old male who sustained polytraumatic injuries in a motor vehicle collision, including a neck seatbelt sign and acute thrombosis of the left subclavian artery adjacent to an undiagnosed hypoplastic cervical rib, presented with a threatened left upper extremity. He underwent emergent surgical exploration through a supraclavicular incision, with cervical rib resection, resection of the contused subclavian artery segment, and end-to-end anastomosis. Through an infraclavicular incision, he had a thrombectomy of the axillary and brachial arteries. Postoperatively, he developed progressive left upper extremity deficits. Imaging revealed proximal axillary and distal subclavian artery dissection with near occlusion, requiring re-exploration and subclavian–axillary bypass using prosthetic conduit to restore distal perfusion. He was discharged on hospital Day 6 on aspirin and anticoagulation. At 5-months, he had no ischemic symptoms, improving fine motor function, and a patent bypass. This case highlights a rare presentation of arterial thoracic outlet syndrome precipitated by blunt trauma.
Introduction
Arterial thoracic outlet syndrome (aTOS) is a rare but limb-threatening condition caused by subclavian artery compression through the thoracic outlet [1], most commonly due to congenital anomalies such as cervical ribs. It typically presents with chronic ischemic symptoms, including upper extremity pain, numbness, pallor, or digital embolization [2–4], while acute presentations are uncommon. Blunt trauma can precipitate arterial thrombosis in patients with predisposing anatomy [5, 6], increasing the risk of distal embolization and limb loss. We present a case of traumatic subclavian artery thrombosis associated with an undiagnosed hypoplastic cervical rib.
Case report
A 39-year-old male with hypertension and type II diabetes mellitus was transferred to our facility after a high-speed, head-on motor vehicle collision with diminished pulses in the left upper extremity. On arrival, he was hemodynamically stable with a Glasgow Coma Scale of 15. Examination revealed a seatbelt sign across the left neck and chest, absent ulnar pulse without Doppler signal, and sensory deficits in the ulnar distribution. Computed tomography angiography (CTA) of the neck and aorta demonstrated a nondisplaced sternal fracture, grade I splenic laceration, and occlusion of the left subclavian artery at the thoracic outlet adjacent to a hypoplastic cervical rib (Fig. 1A and B).
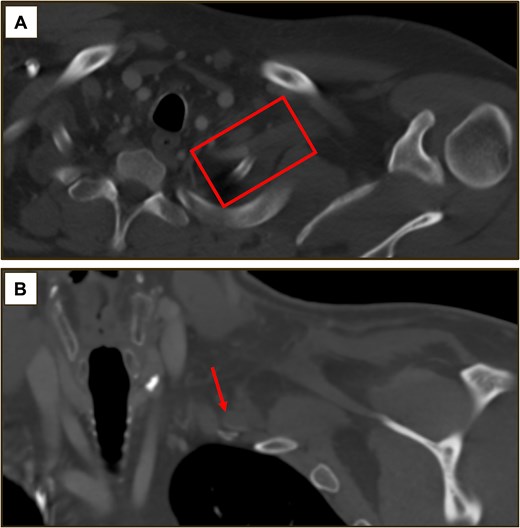
(A) Axial CTA of the neck demonstrating occlusion of the left subclavian artery adjacent to a hypoplastic cervical rib (box). (B) Coronal CTA confirming complete occlusion of the left subclavian artery lumen at the thoracic outlet (arrow).
This patient had evidence of Rutherford IIb acute limb ischemia and necessitated emergent revascularization. He was taken emergently to the operating room for planned open exploration with cervical rib resection and arterial reconstruction. Through a supraclavicular incision, the subclavian artery was exposed to reveal a small segment adventitial hematoma adjacent to the hypoplastic cervical rib. We proceeded with the thoracic outlet decompression by resecting the cervical rib. The patient was then systemically heparinized, and the subclavian artery was clamped proximally and distally. Through a longitudinal arteriotomy, we identified and removed a small volume of clot. The intima and media of the vessel wall were injured, ultimately necessitating resection of 1.5 cm of subclavian artery. A Fogerty catheter was passed distally with adequate back bleeding. Both ends of the vessel were approximated without tension, and end-to-end anastomosis was performed with 6–0 Prolene stitch. Following the repair, Doppler signals were diminished distal to the axilla. Angiogram demonstrated an occlusion 3–4 cm distal to our anastomosis. We proceeded with an infraclavicular exposure of the axillary artery and performed a thrombectomy, restoring a pulse in the left brachial and radial arteries.
Postoperatively, the patient was admitted to the surgical trauma intensive care unit for hemodynamic monitoring and neurovascular checks. He was started on heparin at 500 units/hour. Within a few hours, he developed new motor and sensory deficits–weakness in elbow flexion and extension, loss of grip strength, and an insensate forearm to the level of the elbow. The forearm compartments remained soft without evidence of compartment syndrome. His left radial pulse remained palpable with biphasic Doppler signal in the palmar arch. However, repeat CTA demonstrated dissection of the distal subclavian and proximal axillary arteries with near occlusion (Fig. 2). Given the patient’s neurologic dysfunction, we were concerned that anticoagulation and monitoring alone may not be a reasonable option. After counseling the patient, we urgently returned to the operating room for planned re-exploration and possible bypass. Intraoperative findings were consistent with preoperative imaging, and we performed a left subclavian–axillary artery bypass using prosthetic conduit. We confirmed triphasic signal at the proximal and distal anastomosis and radial artery at conclusion of the case.
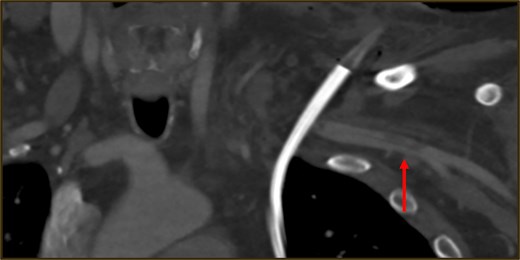
Postoperative CTA following first rib resection, segmental subclavian artery resection, and primary anastomosis demonstrating recurrent intraluminal filling defects (arrow).
After the second operation, the patient’s vascular exam was stable with palpable radial pulse and biphasic Doppler signals in the palmar arch. His neurologic deficits slowly improved with serial occupational therapy assessments; these deficits were ultimately attributed to brachial plexus neuropraxia secondary to the initial ischemia and possible stretch/compression injury from the cervical rib and seatbelt mechanism. Vascular exam of the left upper extremity throughout the remainder of his admission consistently demonstrated palpable radial pulse and biphasic Doppler signals at the palmar arch. The patient was transitioned to dual antithrombotic therapy with aspirin and apixaban. His splenic laceration remained stable, and no abdominal complications developed. After multidisciplinary evaluation by vascular surgery and trauma surgery, he was discharged home on hospital Day 6 with instructions for physical therapy, strict adherence to antithrombotic therapy, and close outpatient follow-up.
At his two-week trauma surgery clinic follow-up, the patient reported improved sensation in the forearm, with partial return of grip strength. He was otherwise asymptomatic and remained compliant with antithrombotic therapy. His one-month surveillance CTA demonstrated a patent graft with persistent, although improving dissection in the distal axillary artery. At 5-months, his imaging was unchanged (Fig. 3). His therapeutic anticoagulation was discontinued and he transitioned to aspirin monotherapy.
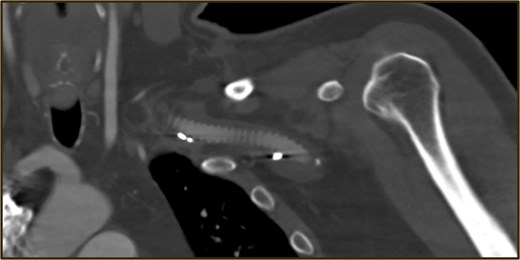
Surveillance CTA after subclavian–axillary artery bypass showing a widely patent graft.
Discussion
TOS is divided into neurogenic, venous, and arterial subtypes, with aTOS comprising 1%–5% of cases. aTOS is typically associated with chronic extrinsic compression of the subclavian artery due to a cervical rib, hypertrophied scalene musculature, or fibrous bands, leading to intimal injury, post-stenotic dilatation, aneurysm, and distal thromboembolism [2–4]. Traumatic aTOS is rare and most often reported with clavicle fractures [7]. This case demonstrates how aTOS may be precipitated by blunt trauma in patients with predisposing anatomy.
Definitive treatment is surgical decompression of the thoracic outlet, however, chronic cases of aTOS may be managed with planned decompression and/or subclavian artery reconstruction. This traumatic presentation required emergent revascularization to salvage limb function. Patients who undergo emergent repairs in the trauma setting remain at high risk for recurrent thrombosis, and subclavian, axillary, and brachial thromboses are a recognized postoperative complication from thoracic outlet decompression [8]. Our patient was likely at higher risk for early re-thrombosis given his trauma-induced hypercoagulable and inflammatory state, combined with his concurrent splenic injury precluding therapeutic anticoagulation. In this case, worsening postoperative ischemic deficits in the left upper extremity prompted urgent surgical re-exploration for subclavian–axillary bypass.
In conclusion, this case raises awareness of the association between blunt trauma and aTOS in patients with unrecognized cervical rib anatomy, which may require emergent decompression and revascularization and carry a higher risk of postoperative thrombosis in the trauma setting.
Author contributions
Each individual listed as an author on this manuscript contributed substantially and in accordance with the guidelines of the International Committee of Medical Journal Editors.
Conflicts of interest
The authors do not have any conflicts of interest to disclose.
Funding
This review did not receive any specific grant from funding agencies in public, commercial, or non-for-profit sectors.
Informed consent
Patient provided written consent for publication of case details.

{kind=link}
{kind=link}
{kind=link}