





Abstract
Intermediate-sized reverse Hill–Sachs lesions (RHSL) occurring in irreducible posterior shoulder dislocations are challenging to manage. Indeed, there is no consensus regarding treatment due to the variety of surgical strategies and the lack of long-term follow-up data. Anatomical reconstruction techniques using allografts may represent a suitable compromise, allowing preservation of bone stock while facilitating recovery of rotational range of motion. We report the 8-year follow-up of two cases of irreducible posterior dislocation treated with fresh-frozen osteochondral allografts. Graft incorporation, potential mechanical complications, and the development of osteoarthritis were assessed using radiography and computed tomography. The survival of these allografts in RHSL remains poorly defined due to the limited long-term data available in the literature.
Introduction
Impaction fractures of the anteromedial articular surface of the humeral head, also referred to as ‘reverse Hill–Sachs lesions’ (RHSL), are rare injuries. These lesions are typically identified following posterior shoulder dislocation and account for the majority of fractures associated with such dislocations [1]. When the defect is too large, posterior dislocation may prove irreducible by closed reduction manoeuvres. In cases of irreducibility, open reduction via arthrotomy is required [2].
The treatment performed in conjunction with reduction depends on the size of the defect. For RHSL involving between 25% and 50% of the humeral head, no standardized treatment currently exists [1]. The three principal therapeutic strategies are external rotation osteotomies, filling techniques (McLaughlin procedure and its variants), and joint reconstruction using bone grafts [1–3]. External rotation osteotomies are less commonly performed due to the high risk of humeral head devascularization and the significant loss of external rotation [1].
Filling techniques and graft-based reconstructions are the most frequently employed procedures; however, their mid- to long-term outcomes remain controversial for intermediate-sized defects. A disadvantage of transferring the lesser tuberosity with the attached subscapularis tendon (original McLaughlin procedure), as well as its variants, is a higher risk of limitation in internal rotation and possible progression to osteoarthritis [4, 5]. Furthermore, transferring the tendon onto the articular surface may compromise the outcomes of any future shoulder arthroplasty [4, 6].
Thus, anatomical reconstruction using bone grafts may represent a suitable compromise, preserving bone stock while restoring rotational range of motion. However, follow-up data for these grafts remain limited to a small number of case series. We report the functional and radiographic outcomes at 8 years of two fresh-frozen osteochondral allografts (FFOCA) used for joint reconstruction of intermediate-sized RHSL in irreducible posterior shoulder dislocations.
Case report
Two patients were treated with FFOCA for RHSL involving approximately 40% of the humeral head in the context of irreducible posterior shoulder dislocation. Their characteristics are summarized in Table 1. The size of the defect (Fig. 1) was estimated using computed tomography according to the method described by Gerber et al. [2]. No additional lesions were associated with the defect.
Patient characteristics.
| Characteristics | Patient 1 | Patient 2 |
|---|---|---|
| Age (years) | 48 | 66 |
| Sex (M/F) | M | M |
| Aetiology | Epilepsy | Epilepsy |
| Timing of management (days) | Chronic (34) | Acute (10) |
| Size of humeral defect (%) | 43% | 42% |
| Allograft used | Fresh-frozen femoral condyle | Fresh-frozen humeral head |
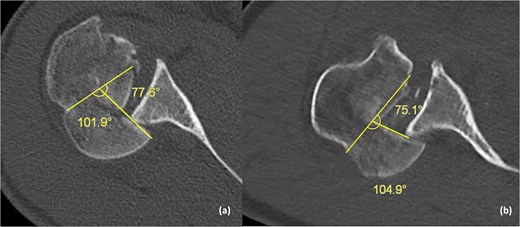
The size of the defect was calculated on an axial CT slice according to the method described by Gerber [2]. The percentage of the lesion corresponds to the ratio between the defect angle (DA) and the cartilage surface angle (CA). The RHSL was estimated at 43% in the first patient (77.6/179.5) (a), and 42% of the articular surface in the second patient (75.1/180) (b).
The first patient underwent surgery 34 days after the initial trauma, as the injury had been missed in the emergency department. The second patient was operated on 10 days after the fall. The surgical technique involved a deltopectoral approach. In the first patient, an osteotomy of the lesser tuberosity was performed. A femoral condyle FFOCA was shaped and fixed using two 4-mm cannulated screws (Fig. 2a). The lesser tuberosity was subsequently reattached using two cannulated screws at the end of the procedure. In the second patient, a subscapularis tenotomy was performed to access the joint. A humeral head FFOCA, fixed with three 4-mm cannulated screws, was used to fill the defect (Fig. 2b). The subscapularis tendon was reinserted using non-absorbable sutures. Immediate postoperative radiographs demonstrated appropriate implant positioning and restoration of the articular surface in both patients (Fig. 3). Early passive mobilization was initiated promptly, with the use of a sling for three weeks.
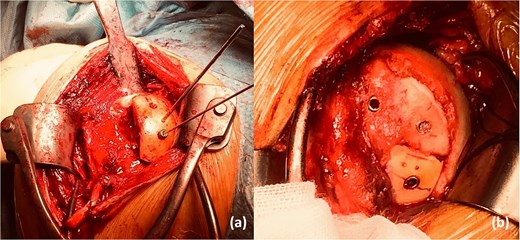
Reconstruction using fresh-frozen osteochondral allografts (FFOCA): femoral condyle (a) and humeral head (b).

Anteroposterior radiographs. In the first patient: Immediate postoperative imaging showing restoration of humeral head sphericity, with no intra-articular screws (a); 8-year follow-up radiograph demonstrating glenoid erosion caused by the hardware (b). In the second patient: Immediate postoperative imaging showing anatomical reconstruction of the humeral head (c); 8-year follow-up radiograph demonstrating incorporation of the humeral head allograft with development of osteoarthritis (d).
The final follow-up was conducted 8 years postoperatively. This assessment included evaluation of shoulder function, graft survival, and potential complications. Functional outcomes were measured using the Constant–Murley Score (CMS) out of 100 points and subsequently adjusted according to age and sex [7]. Radiographic (X-ray) and computed tomography (CT) imaging were performed to assess graft incorporation or partial/complete resorption, detect any implant migration or impingement, and evaluate the presence or absence of osteoarthritis.
Our two patients were reassessed at 104 and 94 months following joint reconstruction, respectively. The total CMS was low in both cases, at 29 and 50.5 points, respectively. The first patient reported no pain but exhibited marked functional impairment, with a negative impact on daily activities. In contrast, the second patient reported intermittent pain but overall preserved mobility. Both patients complained of a significant loss of muscle strength. External rotation was poor in the first patient but acceptable in the second (Table 2). We observed no cases of instability or early or late infection. However, the second patient experienced painful episodes during shoulder mobilization one and a half years after surgery. Investigations revealed impingement of the screw heads against the glenoid. All hardware was removed 22 months postoperatively, resulting in immediate symptom relief (Fig. 4). Radiographs and CT scans obtained at the 8-year follow-up in the first patient demonstrated significant glenoid erosion caused by the screw heads (Fig. 3b), collapse of the femoral condyle allograft, and the development of severe glenohumeral osteoarthritis associated with rotator cuff rupture (Fig. 5a and b). In contrast, the humeral head allograft in the second patient showed good incorporation (Fig. 3d). CT imaging confirmed partial graft resorption, with the development of severe osteoarthritis (Fig. 5c and d). Radiological findings are described in detail in Table 3.
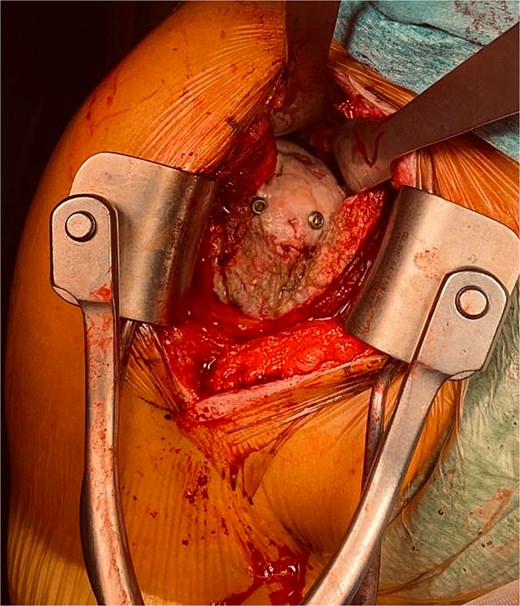
Intraoperative image showing macroscopic incorporation of the humeral head FFOCA in the second patient at the time of hardware removal, 22 months postoperatively. Although the screw heads did not protrude beyond the articular surface at the time of reconstruction (Fig. 2b), they came into contact with the glenoid due to partial graft resorption.
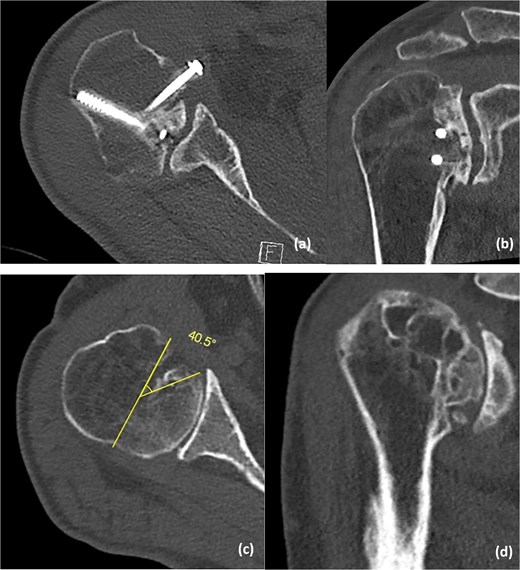
CT scans at 8-year follow-up. In the first patient: Axial view confirming collapse of the femoral condyle allograft (a) and coronal view demonstrating severe glenohumeral osteoarthritis with rotator cuff rupture (b). In the second patient: Axial view showing partial incorporation of the humeral head allograft, with approximately 22% resorption calculated according to Gerber’s method (c), and coronal view demonstrating severe osteoarthritis without rotator cuff rupture (d).
Functional outcomes at 8-year follow-up. Constant–Murley score (CMS).
| Characteristics | Patient 1 | Patient 2 |
|---|---|---|
| Follow-up (months) | 104 | 94 |
| Age (years) | 56 | 73 |
| Pain: 15 points | 15 | 7.5 |
| Mobility | ||
| Anteflexion: 10 points | 4 | 8 |
| Abduction: 10 points | 4 | 6 |
| External rotation: 10 points | 0 | 6 |
| Internal rotation: 10 points | 4 | 4 |
| Activity level: 20 points | 2 | 14 |
| Muscle strength: 25 points | 0 | 5 |
| Total score (out of 100) | 29 | 50.5 |
| Weighted score (%) | 30.85% | 66.44% |
Radiographic outcomes at 8 years following joint reconstruction.
| Characteristics | Patient 1 | Patient 2 |
|---|---|---|
| Type of allograft | Fresh-frozen femoral condyle | Fresh-frozen humeral head |
| Follow-up (months) | 104 | 94 |
| Allograft incorporation (complete or partial) / Collapse or necrosis | No incorporation. Collapse | Partial incorporation. Resorption estimated at 22.5% (DA/CA according to Gerber) |
| Osteoarthritis (OA) | Severe osteoarthritis with rotator cuff tear | Severe centred osteoarthritis |
| Hardware impingement or migration | Glenoid erosion caused by screw head | Painful impingement requiring hardware removal at 22 months postoperatively |
| Revision surgery | Reverse arthroplasty indicated but declined by the patient | None |
No revision surgery was required; however, reverse total shoulder arthroplasty was proposed for the first patient but was declined.
Discussion
The advantage of reconstruction using bone grafts lies in the preservation of glenohumeral anatomy, with restoration of both shoulder stability and mobility. Some authors suggest that these techniques may be superior to so-called ‘non-anatomical’ filling procedures, owing to improved functional outcomes in defects involving 30% to 50% of the humeral head articular surface [8, 9]. However, at present, no clinical difference has been demonstrated between these two approaches for intermediate-sized RHSL, with a higher risk of progression to osteoarthritis reported following anatomical reconstructions [4, 10]. It remains difficult to determine the superiority of any surgical strategy, given the limited number of studies addressing this condition, most of which consist of small case series. The inability to establish clear recommendations is also explained by the heterogeneity of anatomical reconstruction techniques using bone grafts. These include the use of allografts with differing mechanical properties (femoral versus humeral head), various preservation methods (fresh-frozen, cryopreserved, processed, or lyophilized), and sometimes differing underlying aetiologies [4, 10, 11]. In addition, adjunctive techniques are occasionally employed alongside grafting. For instance, Schliemann et al. [12] used cement augmentation in combination with allografts, while Konrads et al. [13] described techniques involving elevation of the intact articular surface combined with autografts. Finally, some authors, such as Gerber et al. have reported the use of iliac crest autografts in five patients [2, 13], whereas the majority of studies describe outcomes using allografts. However, the osteogenic and osteoconductive properties of these two types of bone substitutes differ substantially.
Studies reporting mid- to long-term outcomes of FFOCA used in isolation, without adjunctive techniques, for the management of intermediate-sized defects in irreducible posterior shoulder dislocations remain scarce (Table 4). Diklic et al. [9] and Muccioli et al. [14] reported mid-term results (5 years) for 25 allografts (50% humeral head; 50% femoral head). Only five allografts achieved complete incorporation. The remaining 20 demonstrated either partial incorporation [7], necrosis [1], or progression to mild [10] or moderate [2] glenohumeral osteoarthritis. The CMS ranged from 40 to 97 points, indicating highly heterogeneous outcomes. The absence of weighted scores limits the interpretation of these results. Gerber et al. [2] and Martinez et al. [15] reported the most substantial long-term outcomes, with a follow-up of approximately 10 to 12 years for a total of 20 allografts (14 femoral heads and 6 humeral heads). The authors reported eight cases of osteoarthritis and two cases of graft collapse. Overall, six revision surgeries with shoulder arthroplasty were required, including three prostheses implanted more than 10 years after joint reconstruction. Gerber et al. [2] estimated the lifespan of these allografts to be approximately 15 years. Among the seven cases of osteoarthritis reported by Gerber et al. [2], five occurred in patients with delayed management, defined as more than three weeks after the initial trauma. Although no hardware-related impingement was reported, the authors elected to perform prophylactic screw removal in three patients at 8, 10, and 18 months postoperatively [2]. At 10 years of follow-up, CMS values also remained highly variable, ranging from 40 to 100 points. Only Gerber et al. [2] reported weighted scores, with a mean functional outcome of approximately 89.5% at around 12 years in a series of 14 patients. Overall, among the 45 osteochondral allografts reported, there were 20 cases of osteoarthritis, one case of necrosis, and two cases of graft collapse. The estimated risk of unfavorable long-term outcomes (osteoarthritis, necrosis, or graft collapse) is approximately 51%, corresponding to a one-in-two likelihood [2, 9, 14, 15].
Mid- and long-term functional and radiographic outcomes of fresh-frozen osteochondral allografts used in isolation, without adjunctive techniques, for joint reconstruction of RHSL: retrospective studies.
| Study | Shoulders (M/F) | Mean age (years) | Defect (%) | Timing of surgery (weeks) | Type of allograft | Follow-up (months) | Mean CMS (total and %) | Imaging | Allograft incorporation | OA / collapse / necrosis | Hardware complications | Revision surgery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gerber et al. [2] | 14 | 46.96 | 45.71 (Gerber method) | 9 chronic (>4 weeks) | Fresh-frozen femoral heads | 143.29 | 77.5 (52–98); 89.5% | X-ray | Not reported | 7 OA (5 chronic lesions) | None; 3 prophylactic removals (8, 10, 18 months) | 3 arthroplasties (1 early, 2 > 15 years) |
| Diklic et al. [9] | 13 (10/3) | 42 (36–51) | 25–50 (X-ray method) | 17.14 (8.6–38.6) | 12 Fresh-frozen femoral heads, 1 cryopreserved | 54 (41–64) | 86.8 (43–98); no weighted mean | X-ray | 7 partial collapse; 5 complete incorporation | 1 necrosis | Not reported | Not reported |
| Muccioli et al. [14] | 12 | 54.8 (31–72) | 31 (30–50) (Gerber method) | <3 | Fresh-frozen humeral heads | 66 (24–225) | 82.37 (40–97); no weighted mean | X-ray + CT | Incorporation with ~4% resorption | 10 mild OA; 2 moderate OA | None | None |
| Martinez et al. [15] | 6 (6/0) | 26.42 (22–30) | >40 (Gerber method) | 7.5 (7–8) | Frozen humeral heads | 122 (96–144) | 69.2 (40–100); no weighted mean | X-ray + CT | 3 complete incorporations | 2 collapses; 1 OA | None | 3 arthroplasties |
Furthermore, long-term functional outcomes reported in the literature are particularly heterogeneous. The risk of poor outcome appears to be directly correlated with the delay in initial management. Indeed, functional outcome (66%) was better in our patient treated early compared with the patient whose diagnosis was delayed (30%). According to Gerber et al. restoration of the sphericity of the humeral head is key to achieving favorable long-term functional outcomes [1, 2]. However, in contrast to previously reported cases, our 8-year results highlight a significant risk of hardware-related impingement: glenoid erosion caused by screw heads in the first patient, and painful impingement requiring hardware removal at 22 months in the second patient. Nevertheless, our cohort is small, including only two patients. Moreover, the surgical techniques differed between cases, with a lesser tuberosity osteotomy performed in the first patient and a subscapularis tenotomy in the second, which may have influenced both functional and radiological outcomes.
This study illustrates the functional and radiographic outcomes at 8 years following the filling of RHSL using two FFOCA: one humeral head and one femoral condyle. To our knowledge, unlike the humeral head, the femoral condyle has not previously been used for joint reconstruction in irreducible posterior shoulder dislocations. The poor outcome observed in this patient is likely attributable to the delayed initial management and does not allow definitive conclusions to be drawn regarding the effectiveness of this type of graft. Our findings highlight the importance of early management in achieving satisfactory functional outcomes. We also believe that the heterogeneity of joint reconstruction techniques complicates the interpretation of results reported for bone grafting in the current literature. The use of allografts—and occasionally autografts—with or without adjunctive techniques, and with different preservation methods, may influence both functional outcomes and graft incorporation. However, even when restoration of the humeral head sphericity is achieved, we believe that this technique yields only moderate long-term functional results. The risk of long-term progression to osteoarthritis or graft collapse appears to be approximately one in two. We particularly emphasise the risk of hardware-related impingement against the glenoid, a complication that is likely underestimated in the literature. Even when graft incorporation occurs, partial resorption—variable between cases—remains inevitable, thereby exposing the glenoid to screw head contact. For this reason, we recommend systematic hardware removal at one year following reconstruction in order to prevent glenoid erosion and reduce the risk of early osteoarthritis.
Conflicts of interest
None declared.
Funding
No specific funding was received.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}