





Abstract
Chondromesenchymal hamartoma of the chest wall (CMHCW) is an extremely rare benign tumour-like lesion typically presenting in early infancy, arising from one or more ribs and capable of mimicking malignancy. We report a 4-month-old male infant who presented with an incidentally discovered firm left posterolateral chest wall mass. Contrast-enhanced computed tomography revealed a large heterogeneously enhancing mass centred on the left sixth rib with rib destruction and partial involvement of adjacent ribs, alongside two smaller ipsilateral anterior chest wall lesions—confirming a multifocal unilateral presentation. Percutaneous ultrasound-guided Tru-cut biopsy and subsequent incisional biopsy of all lesions confirmed CMHCW histopathologically. Following multidisciplinary team discussion, staged surgical resection with mesh reconstruction was performed for all lesions, with postoperative histopathology confirming complete excision. The patient remains on regular clinical and radiological follow-up. This case highlights the importance of multidisciplinary evaluation, pre-operative biopsy, and staged surgical resection in multifocal CMHCW.
Introduction
Chondromesenchymal hamartoma of the chest wall (CMHCW), also known as mesenchymal hamartoma of the chest wall, is an extremely rare benign lesion with an estimated incidence of ˂0.03% of all primary bone tumours [1]. Since its initial description in the 1970s, ˂150 cases have been reported in the literature, with the vast majority occurring in neonates and infants during the first year of life [2, 3]. The lesion typically arises from one or more ribs and presents as an extrapleural mass, often with associated rib destruction and a heterogeneous soft tissue component [4].
Despite its benign nature, CMHCW poses a significant diagnostic challenge due to its alarming radiological and histopathological features, which may closely resemble those of malignant chest wall tumours such as Ewing sarcoma, primitive neuroectodermal tumour, or rhabdomyosarcoma [5]. Histologically, the lesion is characterized by a disorganized admixture of cartilaginous nodules, spindle-cell mesenchymal stroma, woven bone, and haemorrhagic cystic spaces reminiscent of aneurysmal bone cysts [6].
A multifocal presentation of CMHCW—defined by the simultaneous occurrence of more than one lesion—is particularly uncommon, having been described in only a handful of published reports [7, 8]. The optimal management of multifocal disease remains undefined, with some authors advocating conservative surveillance and others recommending surgical excision [9, 10]. We report a case of multifocal unilateral CMHCW in a 4-month-old male infant, managed successfully with staged surgical resection and mesh reconstruction, and discuss the diagnostic approach and therapeutic considerations in the context of the current literature.
Case report
A 4-month-old male infant with no significant past medical history was brought to medical attention after his mother noticed a firm mass over the left chest wall. The infant had no history of trauma, fever, respiratory distress, or weight loss. On physical examination, a firm, non-tender mass was palpated over the left posterolateral chest wall. There were no signs of respiratory compromise, and systemic examination was otherwise unremarkable.
Contrast-enhanced computed tomography (CT) of the chest revealed a large left posterolateral chest wall mass centred on the left sixth rib, with cortical destruction of the sixth rib and partial involvement of the adjacent fifth and seventh ribs. The lesion demonstrated heterogeneous enhancement with an extra-osseous soft tissue component measuring ~6.5 × 7.2 × 5.6 cm. Two additional smaller heterogeneously enhancing soft tissue masses were identified along the left parasternal anterior chest wall, measuring ~1.6 × 2.9 × 2.1 cm and 1.6 × 2.1 × 2.0 cm, respectively. There was no pleural effusion or direct pulmonary parenchymal involvement (Fig. 1).
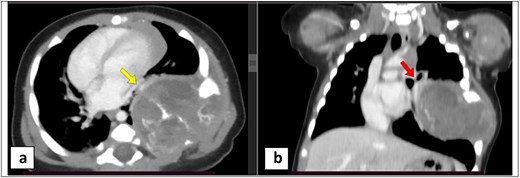
Axial and coronal contrast-enhanced CT images (a, b) show a left posterolateral chest wall complex lesion arising from the left sixth rib, with associated intrathoracic and extrathoracic soft tissue components. The lesion demonstrates multilocular cystic changes, calcifications, and enhancing soft tissue elements. The intrathoracic component causes underlying lung collapse and extends towards the left hilum (red arrow) and pulmonary veins (yellow arrow), without vascular encasement, with mild contralateral mediastinal shift. Extension into the left paravertebral region is noted with no intraspinal involvement.
Given the size of the dominant posterolateral lesion and its imaging characteristics, the patient underwent percutaneous ultrasound-guided Tru-cut biopsy of the left posterolateral chest wall mass. Histopathological analysis demonstrated features consistent with chondromesenchymal hamartoma, including disorganized cartilaginous nodules, spindle-cell mesenchymal stroma, woven bone formation, and haemorrhagic cystic areas (Figs 2 and 3).
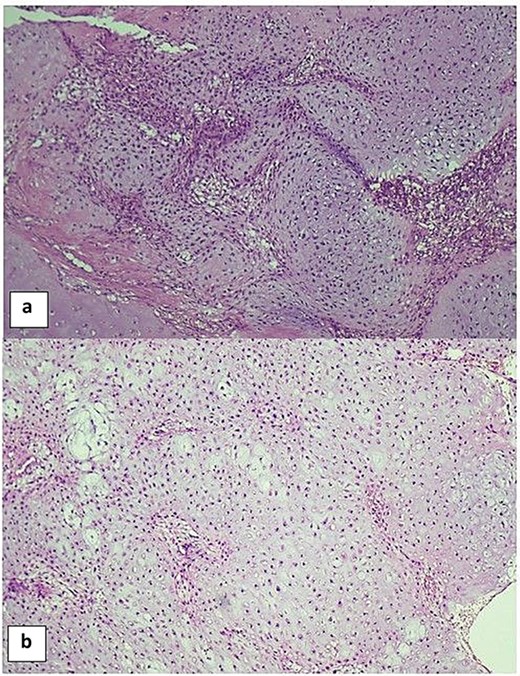
Histopathological features of chondromesenchymal hamartoma showing solid areas composed of lobules of hyaline cartilage with intervening benign spindle cells (a, b) (H&E, ×10).
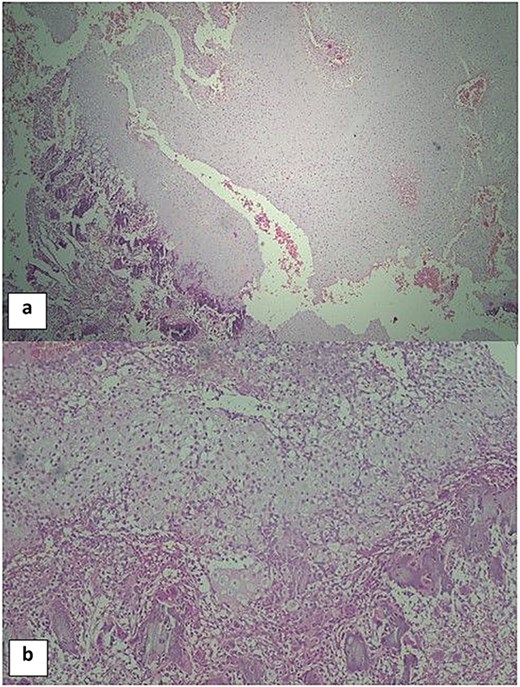
The cystic areas of the lesion demonstrate aneurysmal bone cyst-like features, including haemorrhage and osteoclast-type giant cells, with foci of calcification (a, b) (H&E, ×10).
The case was discussed in a multidisciplinary team (MDT) meeting involving paediatric oncology, paediatric surgery, radiology, and pathology specialists. Given the multifocal nature of the disease and the need to characterize all lesions prior to definitive management, an incisional biopsy was subsequently performed from each of the two anterior chest wall masses (Fig. 4). Histopathological examination of both specimens confirmed chondromesenchymal hamartoma of the chest wall.
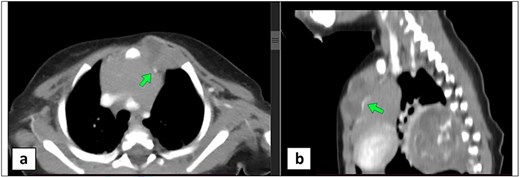
Axial and sagittal contrast-enhanced CT images (a, b) demonstrate an additional multilobulated anterior parasternal chest wall lesion at the level of the first and second costal cartilages, showing multilocular cystic changes and enhancing soft tissue components. The lesion abuts the thymus gland and displaces the left internal mammary vessels (green arrow).
Based on MDT recommendations, the patient underwent surgical resection of the dominant left posterolateral chest wall mass as the first stage of treatment. The resection included the involved rib segments, and chest wall reconstruction was performed using synthetic mesh. Postoperative histopathological examination confirmed complete excision of chondromesenchymal hamartoma with clear margins.
Following further MDT discussion and satisfactory postoperative recovery, the patient subsequently underwent a second-stage surgical resection of the remaining two anterior chest wall lesions. Postoperative histopathology confirmed complete excision of chondromesenchymal hamartoma in both specimens. The postoperative course was uneventful, with no haemodynamic instability or respiratory compromise. The patient is currently on regular follow-up, with ongoing clinical and radiological surveillance demonstrating no evidence of residual or recurrent disease.
Discussion
CMHCW is a rare benign lesion arising from the rib cage in neonates and infants. Its pathogenesis remains unclear, though aberrant mesenchymal differentiation during foetal development is implicated [3, 4]. An association with DICER1 gene mutations has been reported in nasal chondromesenchymal hamartoma, suggesting possible shared molecular mechanisms; however, routine genetic testing is not standard practice [11].
Clinically, CMHCW is variable. Patients may be asymptomatic, as in our case, or may present with chest wall deformity or respiratory distress when the lesion impinges upon the lung or mediastinum [5, 6]. A male predominance is consistently reported [7].
On cross-sectional imaging, CMHCW appears as an expansile, heterogeneously enhancing rib mass with calcification and haemorrhagic cystic components [4, 6]. These features simulate malignant tumours, particularly Ewing sarcoma, making tissue diagnosis essential. Percutaneous image-guided biopsy proved safe and reliable in our case, confirming the benign diagnosis and avoiding radical surgery [12]. Histopathologically, the lesion comprises cartilaginous nodules, spindle-cell stroma, woven bone, and haemorrhagic cystic spaces resembling aneurysmal bone cysts, with no specific immunohistochemical markers [2, 6].
A multifocal presentation, as in our patient, is uncommon. Sodhi et al. described unilateral multifocal CMHCW, and Troum et al. reported bilateral multifocal disease (Table 1) [7, 8]. Management is not standardized. Conservative surveillance may suffice for small, asymptomatic lesions [9]; however, the dominant lesion exceeded 6 cm with extensive rib destruction and progressive risk. Although malignant transformation remains controversial, surgical resection was warranted [3, 13]. Complete resection with clear margins is widely considered curative [2, 5].
Summary of selected published cases of chondromesenchymal hamartoma of the chest wall (CMHCW), including the present case.
| Author (year) | Age / sex | Presentation | Site / ribs involved | Imaging | Diagnosis method | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| Groom et al. (2002) [4] | Neonates & infants (series) | Chest wall mass; some with respiratory distress | Multiple ribs, unilateral | Expansile rib lesion; mineralization; haemorrhagic cysts on CT/MRI | Histopathology | Surgical resection (some conservative) | Benign; no recurrence |
| Andiran et al. (1998) [5] | Infants | Alarming chest wall mass | Rib-based, unilateral | CT: expansile destructive rib lesion mimicking malignancy | Biopsy + histopathology | Surgical resection | Benign course; no recurrence |
| Troum et al. (1996) [8] | Infant / M | Multiple bilateral chest masses | Bilateral multifocal ribs | CT: bilateral expansile rib lesions | Histopathology | Conservative + staged resection | Benign; stable follow-up |
| Sodhi et al. (2009) [7] | Infant / M | Unilateral multifocal chest masses | Unilateral multifocal ribs | CT: multiple heterogeneous rib lesions | Biopsy + histopathology | Staged surgical resection | Complete excision; no recurrence |
| Tsuji et al. (2012) [12] | Neonates / M | Bilateral chest masses; respiratory distress | Bilateral ribs | CT: bilateral expansile rib lesions with soft tissue | Histopathology | Bilateral surgical resection | Uneventful recovery |
| Chua et al. (2019) [9] | 4 months / M | Incidental chest wall mass | Left ribs, unifocal | CT: heterogeneous enhancing rib mass | Percutaneous biopsy + histopathology | Conservative surveillance | Stable; no progression |
| Yavuz et al. (2019) [10] | Newborn / M | Multifocal chest masses | Bilateral ribs | CT: multiple expansile rib lesions | Histopathology | Conservative management | Spontaneous regression |
| Li et al. (2020) [1] | 5 months / M; 24 years / M | Chest wall mass; mediastinal mass | Left 5th–6th ribs; left 5th rib | CT: expansile rib lesion with calcification; MRI: heterogeneous mass | Histopathology | Surgical resection (thoracoscopy in adult) | Uneventful; DIC in infant postop |
| Inserra et al. (2023) [3] | Children (series, n = 5) | Chest wall mass; one bilateral | Unilateral/bilateral ribs | CT: expansile heterogeneous rib lesions | Histopathology | Percutaneous ablation (RFA/MWA/cryo) | Lesion control; no resection needed |
| Present case (2026) | 4 months / M | Incidental firm left chest wall mass | Left 5th–7th ribs (dominant) + 2 anterior parasternal lesions (multifocal) | CT: large heterogeneous mass 6.5 × 7.2 × 5.6 cm + 2 smaller anterior lesions | US-guided Tru-cut biopsy + incisional biopsy | Staged surgical resection + mesh reconstruction | Complete excision; no recurrence on follow-up |
Abbreviations: CT, computed tomography; DIC, disseminated intravascular coagulation; M, male; MRI, magnetic resonance imaging; MWA, microwave ablation; RFA, radiofrequency ablation; US, ultrasound.
A staged approach was adopted, with resection of the dominant lesion and mesh reconstruction performed first, followed by excision of the anterior lesions after recovery. Mesh reconstruction prevented flail chest, a recognized complication of extensive rib resection in infants [3, 10]. Both stages were completed without significant morbidity.
In conclusion, this case highlights the diagnostic challenge of multifocal CMHCW, the value of MDT-guided management, the utility of pre-operative percutaneous biopsy, and the feasibility of staged surgical resection with mesh reconstruction. Clinicians should consider CMHCW when managing chest wall masses in infants to avoid unnecessarily aggressive treatment.
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Ethical approval was not required for this case report. Written informed consent was obtained from the patient’s parents/guardians for publication of this case report and its associated images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}