





Abstract
Dysplasia epiphysealis hemimelica, also known as Trevor’s disease, is a rare developmental disorder characterized by asymmetric epiphyseal osteochondral overgrowth, most commonly affecting the ankle or knee in pediatric patients. Surgical excision is typically indicated when lesions cause deformity, mechanical symptoms, or functional limitation, although recurrence has been reported. We present the case of a three-year-old male with dysplasia epiphysealis hemimelica of the ankle who experienced two recurrences over a five-year period despite apparently complete surgical excision confirmed intraoperatively. The patient ultimately required three operative procedures due to progressive gait disturbance, stiffness, and pain with ambulation. This case demonstrates the potential for repeated recurrence in skeletally immature patients and highlights the importance of symptom-guided management and long-term surveillance in pediatric patients with dysplasia epiphysealis hemimelica.
Introduction
Dysplasia epiphysealis hemimelica (DEH) is a non-hereditary developmental disorder characterized by unilateral epiphyseal osteochondral overgrowth, most commonly affecting the lower extremity [1–3] , although involvement of the upper extremity has also been reported [4, 5]. DEH has an estimated incidence of ~1 per 1 000 000, with typical onset between two and eight years of age and a reported male predominance [6]. Unlike conventional osteochondromas, which arise from the metaphysis, DEH lesions originate from the epiphysis [7]. The pathogenesis is not fully understood but is thought to involve abnormal cartilage proliferation during early skeletal development, possibly related to disruption of the apical ectodermal cap [8]. Azouz et al. classified DEH into three forms: localized (involving a single epiphysis), classic (involving multiple epiphyses within the same limb), and generalized (involving the entire lower extremity) [9].
The clinical presentation of DEH is often non-specific and may include pain with activity, impaired gait mechanics, limited joint motion, and visible deformity from mass effect [6]. Initial diagnosis is typically made with radiographs demonstrating an epiphyseal osteocartilaginous mass, while computed tomography and magnetic resonance imaging (MRI) are useful for surgical planning and evaluation of surrounding soft tissue and osseous structures [10]. Histologic findings are not specific and may resemble isolated osteochondroma, while genetic testing usually demonstrates normal expression of EXT1 and EXT2 tumor suppressor genes, helping differentiate DEH from hereditary multiple exostoses [11]. There is no effective medical therapy, and surgical excision of symptomatic lesions and loose bodies remains the mainstay of treatment to prevent progressive deformity and degenerative joint changes [2, 12]. A recent review of 70 patients by Artioli et al. reported recurrence in ~9% of cases following surgical excision [2].
Despite growing awareness of DEH, there remains no clear consensus regarding long-term management or the duration of follow-up, particularly in skeletally immature patients. While recurrence following excision has been reported, guidance on surveillance until skeletal maturity remains limited. We present a pediatric case of classic ankle DEH with two recurrences over five years requiring three surgical excisions, highlighting the potential for repeated osteochondral proliferation prior to skeletal maturity and the need for careful longitudinal follow-up and patient counseling.
Case report
Initial presentation
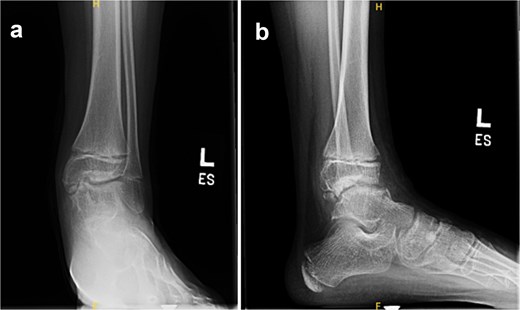
A three-year-old male presented to clinic for evaluation of abnormal appearance of the left foot. Examination revealed in toeing, tibial torsion, hindfoot valgus, pes planus, and a palpable bony prominence along the medial malleolus. He had no significant past medical history. Radiographs of the left ankle demonstrated osteochondral irregularities involving the medial talar dome and medial cuneiform (Fig. 1). MRI further identified five osteochondromas: three arising from the medial talus and two from the medial navicular, confirming the diagnosis of DEH.

AP ankle (a), AP foot (b), and lateral ankle (c) radiographs demonstrating osteochondral irregularity of the talar dome with disruption of the ankle mortise and flattening of the medial longitudinal arch.
Initial surgical treatment
Surgical excision was performed through a curvilinear anteromedial ankle incision. Osteochondromas from the talus and navicular were removed, and fluoroscopy confirmed complete resection. An additional distal tibial epiphyseal osteochondroma not seen on preoperative imaging was identified and excised intraoperatively. The postoperative course was uncomplicated aside from mild wound dehiscence.
First recurrence
At 9-month follow-up the patient remained asymptomatic, although radiographs demonstrated recurrent ossification along the talus. Pes planus and hindfoot valgus persisted with weightbearing, and management consisted of observation. Fifteen months after the index procedure, the patient returned with pain during ambulation and a limping gait. Imaging demonstrated progression of osteochondral growth involving the talus and distal tibia with intra-articular loose bodies in the tibiotalar joint (Fig. 2).

Preoperative AP (a), mortise (b), and lateral (c) ankle radiographs obtained prior to the second surgery demonstrating osteochondromas and irregularity involving the talar dome and distal tibia.
Second surgical treatment
A second excision was performed 18 months after the index procedure. An anterior approach was used to remove talar osteochondromas and a loose osseous body, while a posterior curvilinear incision allowed removal of additional lesions from the posterior talus. Fluoroscopy confirmed complete resection. Distal tibial osteochondromas identified on imaging were not excised because they were not producing mechanical symptoms and resection near the distal tibial physis carries risk of growth disturbance in skeletally immature patients. The patient recovered without complications.
Second recurrence
Approximately three years after the index procedure, the patient demonstrated gait abnormalities including decreased subtalar motion and persistent pes planovalgus deformity but remained active without functional limitation. Serial radiographs demonstrated progressive osteochondromas involving the talus and talonavicular joint with ossification of the medial cuneiform and medial malleolus (Fig. 3). Given minimal symptoms, management remained observational. Approximately five years after the initial surgery, the patient developed worsening ankle stiffness and dorsal ankle pain with functional limitation, prompting consideration of repeat surgery.

Preoperative AP and lateral ankle (a and b) and foot (c and d) radiographs demonstrating progression of DEH with talar osteochondromas and irregularity of the navicular–medial cuneiform articulation.
Third surgical treatment and outcome
A third excision was performed through the same anteromedial approach. A single osteochondroma measuring ~1 cm was identified and excised from the subtalar joint (Fig. 4). Fluoroscopy confirmed complete removal and no additional loose bodies were identified. Postoperative radiographs demonstrated persistent irregularity of the distal tibia and talus with residual osteochondral changes consistent with postoperative remodeling (Fig. 5). No postoperative complications occurred. At 3-month follow-up in early 2026, the patient was recovering well and had begun structured physical therapy. Symptoms had improved compared with earlier in the disease course, although recurrence remains possible given continued skeletal immaturity.
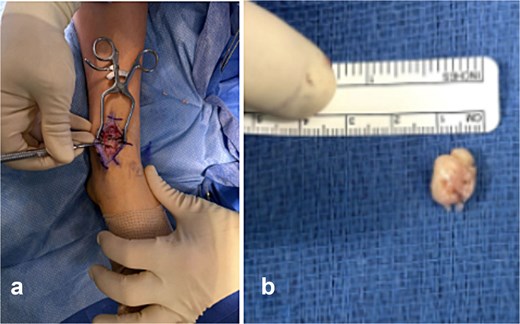
Intraoperative images from the third procedure demonstrating the talar osteochondroma in situ causing mechanical impingement of the ankle (a) and the excised 1-cm lesion with measurement (b).
Postoperative AP (a) and lateral (b) radiographs of the left ankle demonstrating persistent irregularity of the distal tibia and talus with residual osteochondral changes following the third excision.
Discussion
DEH is an uncommon developmental disorder characterized by asymmetric epiphyseal osteochondral overgrowth with highly variable clinical behavior. Although surgical excision remains the primary treatment for symptomatic lesions or those causing joint deformity, outcomes are inconsistent and recurrence may occur. A review by Artioli et al. reported recurrence in ~9% of 70 patients following excision [2]. In contrast, our patient experienced two recurrences over a five-year period despite apparent complete excision confirmed intraoperatively, demonstrating a more aggressive pattern than typically reported.
The etiology of recurrence in DEH remains unclear. One proposed explanation is continued pathological cartilage proliferation in skeletally immature patients with open physes [12]. In this case, recurrence occurred at the talus on two separate occasions while the patient remained skeletally immature, supporting the possibility that abnormal epiphyseal growth may persist alongside normal skeletal development. Surgical intervention was therefore guided by clinical symptoms rather than radiographic progression, with surgery performed once functional limitations developed. However, even with careful resection and intraoperative fluoroscopy, complete removal of cartilaginous components may be difficult to achieve, and incomplete excision has been proposed as a cause of recurrence [13].
Repeated surgical intervention in skeletally immature patients must also be balanced against potential long-term complications. Persistent joint incongruity or stiffness following multiple procedures may predispose patients to early degenerative arthritis [14]. In severe cases, procedures such as tibiotalar or subtalar arthrodesis have been described as salvage options [15]. However, these procedures remain undesirable in young patients and are typically reserved for advanced deformity or refractory symptoms.
Conclusion
DEH remains a challenging condition in pediatric orthopedics due to its unpredictable course and clinical rarity. This case demonstrates that recurrence may occur multiple times despite apparently complete surgical excision, particularly in skeletally immature patients with open physes. Management should prioritize preservation of joint anatomy while balancing the need for surgical intervention against the risks of repeated procedures. Shared decision making and counseling regarding the potential for recurrence are essential, as DEH should be managed as a chronic condition requiring longitudinal follow-up rather than a single surgically correctable pathology.
Conflicts of interest
There are no conflicts of interest. The authors of this paper certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interests in the subject matter or materials discussed in this manuscript.
Funding
No funding was received for this case report.
Ethical statement
The patient was informed that data from the research would be submitted for publication, and consent was obtained.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}