





Abstract
BariClip gastroplasty is an emerging bariatric technique designed to preserve gastric anatomy while providing restrictive weight loss. While preliminary reports have shown promising outcomes, the variety of complications remains incompletely defined. We report the case of a woman in her late 40s with BMI > 35 and a medical history of hypothyroidism, who underwent elective BariClip placement as a primary bariatric intervention. On the second postoperative day, she presented with abdominal discomfort, nausea, and distention. A computed tomography scan revealed inferior slippage of the BariClip and esophageal hematoma. Diagnostic laparoscopy confirmed migration of the device with associated multiple perforations along the gastric wall. The clip was removed, and the perforations were repaired by primary suturing. On the first postoperative day of the secondary operation, the patient developed acute dyspnea and was diagnosed with pulmonary embolism, treated with therapeutic anticoagulation, and discharged home in good condition on postoperative Day 10.
Background
Obesity is a global health crisis, associated with significant comorbidities and increased mortality. Although multiple options such as lifestyle modifications, dietary restrictions, and pharmacotherapy have been extensively investigated, bariatric surgery remains the most effective therapeutic modality for achieving sustained weight loss and metabolic improvement [1].
Laparoscopic vertical clip gastroplasty with the BariClip is a relatively new surgical approach that has shown promise as a safe and minimally invasive technique. This technique involves placing a nonadjustable silicone-coated titanium clip parallel to the lesser curvature of the stomach, generating a restrictive effect comparable to that of sleeve gastrectomy [2].
We present a rare case of early BariClip slippage complicated by gastric perforation, contributing to the limited literature on serious postoperative risks.
Case presentation
A woman in her late 40s with type 2 obesity (BMI 36.3 kg/m2) and hypothyroidism was referred for surgical management of obesity. Following a comprehensive multidisciplinary evaluation, she was a suitable candidate for a bariatric procedure. After discussing the surgical options, the patient elected to proceed with the BariClip procedure, citing its reversibility and preservation of gastric anatomy as motivating factors.
Surgical procedure
Under general anesthesia, the procedure was performed laparoscopically using a five-port technique with a 36-Fr bougie for gastric calibration.
A 36-Fr orogastric bougie was introduced to calibrate the gastric lumen. The BariClip device, composed of titanium arms and a silicone band, was introduced through a 12-mm trocar and applied vertically along the lesser curvature, about 4 cm proximal to the pylorus and extending toward the angle of His. Dissection along the greater curvature was performed carefully to allow proper BariClip placement. Minimal dissection was done at the angle of His to preserve vascular supply, with preservation of the short gastric vessels, no extensive fundus mobilization, and conservative handling of the perigastric fat pad to maintain tissue integrity and reduce ischemia risk.
After locking the clip in place, the bougie was withdrawn. The procedure was accomplished without intraoperative complications, with an overall operative time of 75 min and estimated blood loss of < 70 ml. The patient was extubated and transferred to the surgical floor in stable condition.
Preoperative upper gastrointestinal endoscopy was not performed because the patient was asymptomatic and had no clinical indications. The BariClip device was placed laparoscopically following the manufacturer’s standard technique, without additional fixation methods such as suturing or reinforcement.
Postoperative course
On postoperative Day 2, the patient developed epigastric pain, nausea, and abdominal distention, with stable vital signs and localized tenderness without peritonitis. Labs showed leukocytosis (12 300/μl) with normal lactate. Contrast-enhanced computed tomography (CT) demonstrated inferior BariClip displacement with pneumoperitoneum, suggesting migration and gastric perforation (Figs 1–3).

Hyperdense linear structure seen in the mid-upper abdomen represents the BariClip.
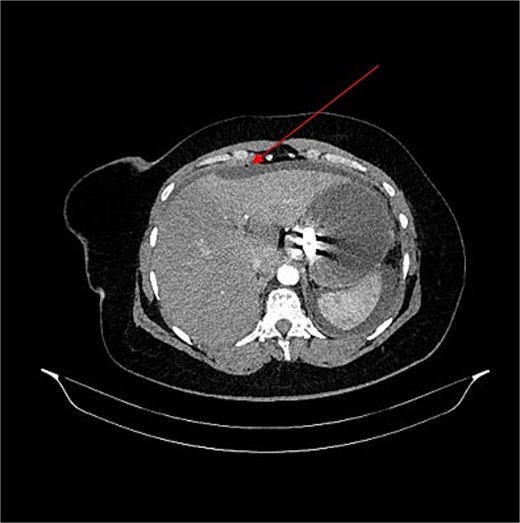
Arterial phase axial CT scan through the upper abdomen shows the gastric clip lying along the lesser curvature of the stomach. The stomach is distended with abdominal ascites and a focus of pneumoperitoneum (arrow). Overall appearances are consistent with a slipped gastric clip, which can cause gastric outlet obstruction and perforation.
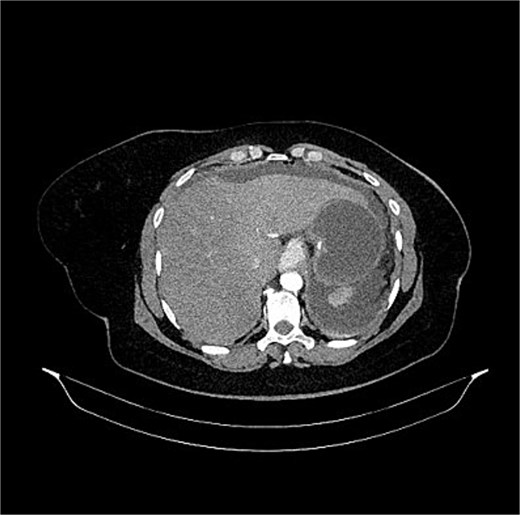
Further foci of pneumoperitoneum seen in the abdominal cavity in keeping with visceral perforation.
Urgent laparoscopy confirmed inferior and posterior clip migration causing pressure necrosis and perforation along the greater curvature (Fig. 4). The device was removed, gastric defects were repaired with interrupted 3-0 polyglactin sutures, followed by peritoneal irrigation and drain placement.
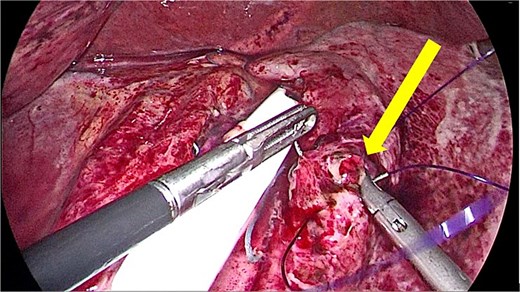
Intraoperative findings of the second surgery showing the slippage and gastric wall perforation, which was repaired using primary suturing (arrow).
Postoperatively, she was admitted to the intensive care unit. On Day 1, she developed acute dyspnea and hypoxemia; CT pulmonary angiography revealed bilateral segmental pulmonary emboli, and therapeutic enoxaparin (1 mg/kg twice daily) was initiated. She remained hemodynamically stable.
The patient was kept NPO for 5 days and received intravenous piperacillin-tazobactam. The drain was removed on Day 6, oral intake resumed on Day 7, and recovery was otherwise uneventful. She was discharged on postoperative Day 10 on anticoagulation, with surgical and hematology follow-up. At 1 month, she was asymptomatic with no recurrent gastrointestinal or thromboembolic complications.
Discussion
BariClip, or laparoscopic vertical clip gastroplasty, is an emerging anatomy-preserving bariatric procedure using a silicone-covered, nonadjustable titanium device placed vertically along the greater curvature and sutured to the gastric wall to restrict food passage while maintaining gastric anatomy and vascularization [3, 4].
It offers advantages such as reversibility, potential gastroesophageal reflux disease (GERD) improvement, absence of malabsorption, and no need for adjustment, with modified techniques proposed to reduce slippage and erosion [3, 4]. Recent studies report a mean operative time of 47 ± 14 min [3], shorter than sleeve gastrectomy (56.9 ± 14.2) and gastric bypass (73.2 ± 20.2) [5], which is an important consideration in surgical risk evaluation.
BariClip showed promising safety and effectiveness compared to other bariatric procedures with a weight loss up to 60% on 5 years follow-up period; Bonaldi et al. (2024) reported a mean total weight loss of 22.6% after a minimum 6-month follow-up period, but reported a high rate of weight regain postoperatively [3]. The reported complications related to BariClip surgery are: bleeding, slippage which was classified by Noel et al. (2023) [6] according to the timing and the position of the slippage (Supplementary Tables SS1 and SS2), and erosions which are highly concerning and are contributed to the chronic slippage, Bonaldi et al. (2024) reported 1 case that suffered from perforation in his study that evaluated the outcomes of BariClip in 69 patients, another case report was identified [7]. Only a minority of the patients experienced local inflammation (<1%), and some studies reported temporary worsening of GERD symptoms [3, 8] Supplementary Tables SS1 and SS2.
In our case, the slippage is classified as type 1B, which is a rare finding. Previous literature noted type 1A slippage as the most common type (up to 90%) of acute slippage occurring in early postoperative days [8], and the standard treatment is removal of the clip. This complication is rare, and overall, it was reported in ~5% of cases in previous studies, with a declining trend due to the fixation modification techniques [3, 4] Supplementary Table SS3. Management of BariClip slippage depends on the severity of displacement and clinical presentation. Minor slippage without perforation or obstruction can be managed conservatively with symptomatic treatment and close follow-up, with endoscopic or radiologic monitoring in selected cases. Moderate cases may require surgical repositioning, especially if symptoms persist or worsen. Major slippage, particularly when associated with complications such as gastric perforation, obstruction, or ischemia, requires prompt surgical intervention, typically involving laparoscopic clip removal and repair of any gastric injury [3, 4, 6, 8, 9]. These findings highlight the importance of early recognition, risk stratification, and timely escalation of management to prevent morbidity.
Sleeve gastrectomy and gastric bypass remain the most commonly performed bariatric procedures. Meta-analyses demonstrate significant weight reduction and metabolic improvement compared with medical therapy, although with higher complication rates [10].
Conclusion
This case describes a rare but serious complication of BariClip gastroplasty involving device slippage with gastric wall perforations requiring urgent surgical intervention. Although the procedure offers anatomical preservation and reversibility, significant mechanical and postoperative complications can still occur. Early recognition of clinical deterioration, prompt imaging, and timely surgical management are essential to reduce morbidity. Further research is needed to better define the safety profile of BariClip and to establish standardized approaches for patient selection, monitoring, evaluation, and complication management.
Learning points/take-home messages
- (1)
Early BariClip slippage can result in gastric perforation and requires prompt surgical management.
(2) Early postoperative abdominal symptoms should prompt immediate imaging evaluation.
Acknowledgements
We would like to thank Dr Rasha Al-Ebbini at King’s College London NHS Foundation Trust for her valuable evaluation of the CT imaging and for providing the detailed notes.
Conflicts of interest
All authors declare that they have no conflict of interest.
Funding
None declared.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}