





Abstract
Mycotic aortic aneurysms pose a unique surgical challenge, with operative management dependent on patient factors and institutional capabilities. In an infected surgical field, cryopreserved aortic homograft (CAH) can provide a durable and infection-resistant repair. We present the case of a 48-year-old male with a mycotic abdominal aortic aneurysm, confounded by an initial diagnosis of blunt abdominal aortic injury. Endovascular aneurysm repair was performed; however, subsequent rapid mycotic degeneration elucidated an infectious component. The patient then underwent explantation of the infected graft with in-line reconstruction via CAH. He has demonstrated clinical stability and graft patency at 16 months postoperatively.
Introduction
Mycotic aortic aneurysm is a rare and life-threatening pathology that necessitates prompt diagnosis and treatment. Definitive management includes excision of the infected tissue, aortic reconstruction, and prolonged antibiotic therapy. In an infected field, cryopreserved aortic homograft (CAH) is an option for in-line aortic repair.
We present a case of a mycotic abdominal aortic aneurysm in a 48-year-old male. Initially diagnosed with blunt aortic injury following a fall, the patient first underwent endovascular aneurysm repair (EVAR). The mycotic component was elucidated postoperatively, eventually requiring open reconstruction with CAH. This case highlights a unique surgical problem: mycotic aortic aneurysm in the presence of infected endograft.
Case report
Patient is a 48-year-old male with history including obesity (BMI 42 kg/m2), type 2 diabetes mellitus (A1c 7.8%), myocardial infarction, hypertension, hyperlipidemia, stage three chronic kidney disease, and schizophrenia. Six days after falling down a staircase, he presented to an outside emergency department with back pain. Non-contrast computed tomography (CT) demonstrated nonspecific retroperitoneal stranding around the infrarenal aorta without aneurysm, hematoma, or disruption. He was discharged with analgesia and instructed to follow up with primary care.
Ten days after, the patient presented to our hospital with persistent back pain and new intermittent bilateral lower extremity weakness and paresthesia. CT angiography (CTA) revealed a 3.4 × 1.6 cm infrarenal aortic pseudoaneurysm (Fig. 1). He proceeded emergently to the hybrid operating room for EVAR. A 23 × 14.5 × 140 mm Excluder Endoprosthesis was deployed in infrarenal position via percutaneous left femoral arterial access. Accompanying 16 × 110 mm limb (GORE Medical, Newark, DE) was deployed via percutaneous right femoral arterial access. A Q50 angioplasty balloon (Merit Medical, South Jordan, UT) was inflated to ensure proper apposition. Completion aortography confirmed appropriate position without endoleak. He was discharged in stable condition on postoperative day (POD) 3.
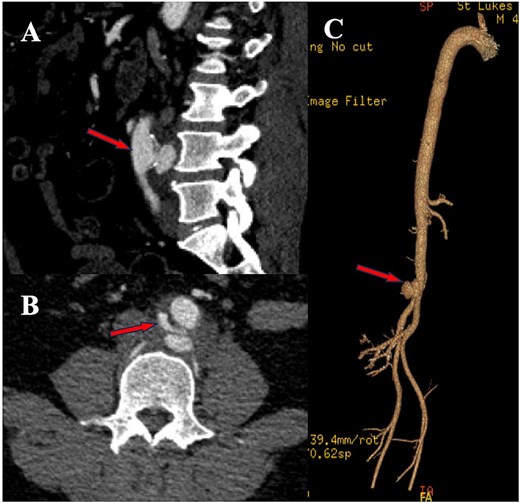
CTA images from initial presentation, demonstrating 3.4 × 1.6 cm posterior infrarenal aortic pseudoaneurysm (indicated by arrow). (A) Sagittal and (B) axial cuts of CTA, with (C) 3D aortic reconstruction.
On POD 13, the patient re-presented with hematuria, lower back pain, and euglycemic diabetic ketoacidosis. CTA demonstrated mild cystitis and bilateral renal cortical hypodensities suggesting infarction versus infection. The endograft was patent, with hypodensity surrounding the distal abdominal aorta concerning for infection versus expected postoperative changes (Fig. 2). On hospital day 4, the hematuria and ketoacidosis had resolved, yet he was persistently tachycardic with new onset fever. Admission blood cultures were negative. Patient refused additional infectious workup and left against medical advice.
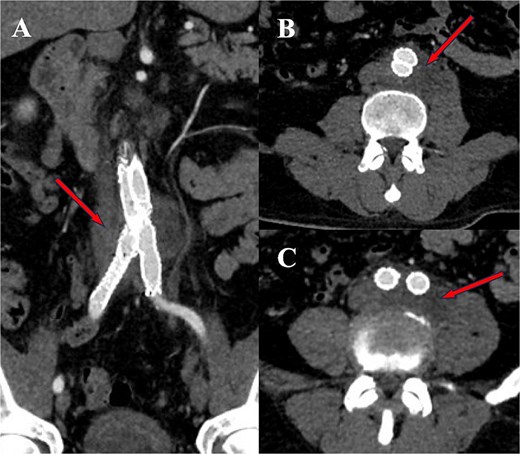
CTA demonstrating mycotic aneurysm and infected collection, indicated by arrows. (A) Coronal slice, (B and C) axial slices.
On outpatient POD 23 follow-up, the patient was tachycardic (140 bpm) and febrile (38.2°C); he was subsequently readmitted. Blood cultures grew Salmonella species and Finegoldia magna. CTA showed enlargement of the aortic sac without contrast extravasation, suggesting endoleak versus abscess.
The patient was taken to the operating room for exploratory laparotomy. Periaortic phlegmon and a psoas abscess were debrided and drained. Proximal aortic control via 7 min of suprarenal clamping and distal control were obtained. The infected endograft was explanted (Fig. 3A). A 10 mm cryopreserved aortoiliac homograft (CryoLife, Kennesaw, GA) was implanted as an anatomic interposition graft with left graft external iliac artery (EIA) (graft hypogastric oversewn) anastomosed to left common iliac artery (CIA) and right graft EIA (graft hypogastric included bevel) anastomosed to right CIA (Fig. 3B). Patient was admitted to the intensive care unit.
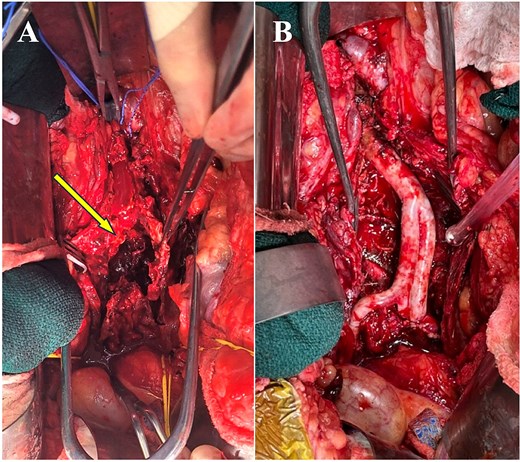
Intraoperative images demonstrating (A) mycotic aneurysm cavity post-removal of infected endograft (indicated by arrow) and (B) cryopreserved arterial homograft post-implantation.
Intraoperative cultures returned Salmonella species. Postoperative course was uneventful, and he was discharged on POD 9. He completed 6 weeks of IV ampicillin, with transition to lifelong oral cefdinir. He has remained well at 16-month follow-up, with 12-month CTA demonstrating patent graft (Fig. 4). Future management includes yearly exams with aortoiliac imaging. Figure 5 details temporality of presentations and surgical interventions.
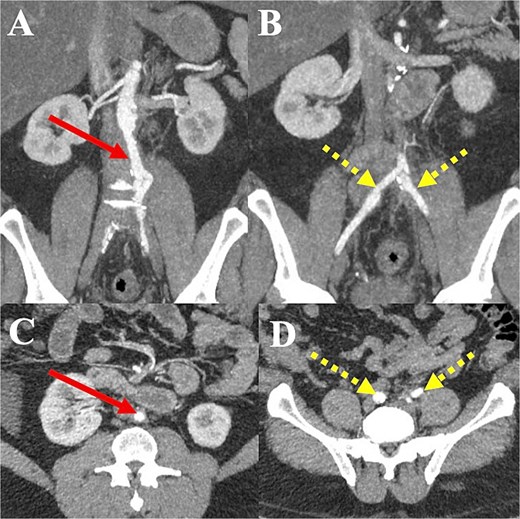
CTA images one year postoperatively. (A and C) Patent aortic graft (indicated by solid arrow) in coronal and axial imaging, respectively. (B and D) Patent iliac limbs of aortic graft with preserved distal flow (indicated by dotted arrow) in coronal and axial imaging, respectively.
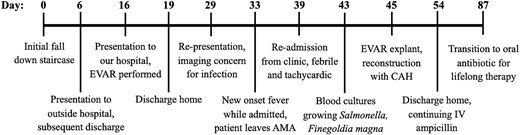
Timeline illustrating patient’s presentations and subsequent interventions. AMA, against medical advice; IV, intravenous.
Discussion
Initially, the patient was diagnosed with blunt abdominal aortic injury (BAAI) and treated endovascularly. BAAI has been reported in <0.1% of trauma admissions with overall mortality of 28% [1, 2]. Presentation may include abdominal or back pain, decreased femoral pulses, neurological defects, or intestinal angina [3]. Treatment options include endovascular and open repair, with reportedly nonsignificant difference in mortality risk [1].
Although the mycotic aneurysm was likely present at the initial blunt injury, we consider the possibility of bacterial seeding via traumatic aortic disruption or a primarily infected prosthetic EVAR graft. However, Salmonella rather than Staphylococcus or Streptococcus species as the causative pathogen supports a diagnosis of primary mycotic aneurysm [4–6]. The patient reported potential Salmonella exposure, with consumption of reportedly undercooked chicken with subsequent gastrointestinal symptoms prior to initial presentation.
For primary aortic or graft infections, reconstruction options include extra-anatomic bypass or in-line reconstruction with CAH, silver coated or antibiotic impregnated (classically rifampin-soaked Dacron) protheses, or neo-aortoiliac system (NAIS) using autogenous femoral veins [7–9]. Extra-anatomic bypass grafting with removal or exclusion of the infected area is a widely accepted treatment option. However, this approach requires prolonged operative time, carries the risk for fatal aortic stump blowout, and has 3-to-5-year patency rates between 43% and 73% [10–13].
Studies assessing CAH for aortic reconstruction have been promising, with 3-year patency rate of 97%, 1-year survival of 75%, and 5-year survival of 51%. Complication rates at 5 years have been reportedly low, with graft-related complications, graft explant, and limb loss of 20%, 12%, and 3%, respectively [9].
The NAIS procedure, performed infrequently and generally at larger institutions, has the advantage of using native conduit, but has been associated with significant morbidity (20% re-intervention rates, 6% re-infection rates) and 9% 30-day mortality [8].
When compared to CAH, antibacterial-loaded prostheses have been associated with lower re-intervention rates but trend toward greater risk for infection reoccurrence. Regardless, 30-day and 5-year mortality have been shown to be not significantly different [14, 15].
This case details the diagnosis and management of a rarity in vascular surgery: mycotic aortic aneurysm with infected aortic endograft in place. The patient’s aortic injury, initially presumed to be secondary to his blunt abdominal trauma, was treated endovascularly. In retrospect, a mycotic aneurysm was likely present at this time. The diagnosis, especially in patients with relevant potential exposures such as Salmonella via undercooked poultry, should be considered to allow for timely repair. Strategies for operative intervention take into consideration patient factors, surgeon experience, and institutional capabilities. For aortic reconstruction in the setting of highly virulent organisms or frank purulence, cryopreserved homograft has seen favorable outcomes and should be considered.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}