





Abstract
Neuroendocrine tumors such as pheochromocytoma and paraganglioma lead to inappropriate release of catecholamines. A 50-year-old woman presented with a para-aortic paraganglioma as a well-defined hypervascular left para-aortic soft tissue lesion measuring 4.1 × 4.2 × 4.5 cm and elevated plasma/urinary fractionated metanephrines. This case highlights the importance of the systematic approach in managing rare neuroendocrine neoplasms, starting with having a low threshold of consideration of pheochromocytoma and paraganglioma for early detection, tight control of symptoms, appropriate medical and surgical intervention, and routine postoperative follow-up.
Introduction
The neuroendocrine neoplasms that develop in the chromaffin cells of the autonomic nervous system, known as pheochromocytoma (PCC) and paraganglioma (PGL), are rare adrenergic-secreting tumors. PCCs are defined as tumors that originate from the adrenal medulla, whereas PGLs arise from extra-adrenal paraganglia [1]. The incidence of PCC and PGL ranges between 2 and 8 per million [2]. The diagnosis can be established through urine/plasma chemistry tests for catecholamines and metanephrines, and the confirmation is achieved through imaging studies such as adrenal computed tomography (CT) scans, T2-weighted magnetic resonance imaging, or 123-I metaiodobenzylguanidine (MIBG) scintigraphy [3].
The rarity of PGLs, particularly in locations such as the para-aortic regions, makes them unique at presentation, and it is important to report the best surgical approach to treat them and the postoperative course; hence, in this case report, we describe a 50-year-old female patient who presented with difficult-to-control hypertension. Further investigation revealed a para-aortic mass, which was ultimately diagnosed as a PGL.
Case report
A 50-year-old female patient with a known case of hypertension had multiple emergency department visits for a hypertension emergency. She was on 5 medications to control her blood pressure. The abdominal examination did not reveal any masses, and a neurological assessment showed no deficits. The patient was investigated for resistant hypertension. The work-up included abdominal ultrasound, which revealed a para-aortic mass 4.6 × 3.1 cm in size. The patient had elevated serum catecholamines (Metanephrine: 88 pg/ml (reference range: <57 pg/ml), norepinephrine: 3346 pg/ml (reference range: 80–520 pg/ml), and high urinary fractionated metanephrines 33.69 μmol/day (reference range: 0.00–3.43). CT scan of the abdomen and pelvis with intravenous contrast revealed the following:
A well-defined hypervascular left para-aortic soft tissue lesion with few low-attenuating components measuring 4.1 × 4.2 × 4.5 cm in the anteroposterior, craniocaudal, and transverse dimensions was observed (Fig. 1). Delayed total body images and the SPECT CT demonstrate intense MIBG avid mass at the left paraaortic region measuring 4.5 × 3.9 × 4.3 cm (AP × TR × CC). No MIBG with avid nodal or distant metastases was observed (Fig. 2). Surgical intervention was selected. The endocrinology team was consulted, and they kept her on metoprolol 5 mg, amlodipine 5 mg, and terazosin 2 mg daily. The patient showed optimal blood pressure readings without orthostatic drop. She was admitted to the hospital 5 days before the surgery for blood pressure control.
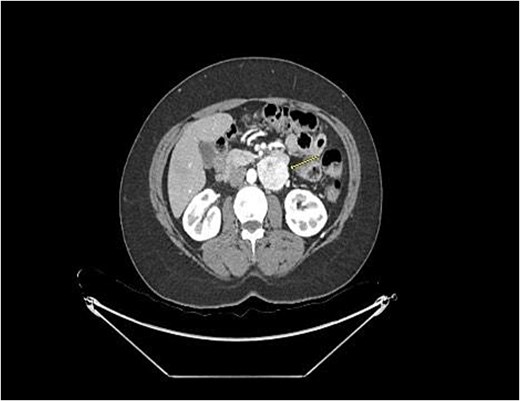
CT scan revealed a well-defined hypervascular left Para-aortic soft tissue lesion with few low attenuating components measuring 4.1 × 4.2 × 4.5 cm in the anteroposterior, craniocaudal, and transverse dimensions.
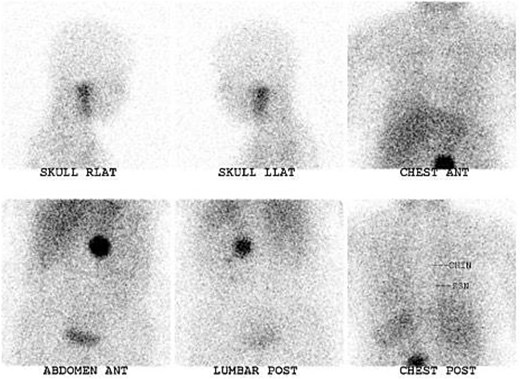
Intense MIBG avid mass at the left para-aortic region measuring 4.5 × 3.9 × 4.3 cm (AP × TR × CC).
Upon admission, the patient was within the target blood pressure range. The procedure was initiated with intravenous isotonic normal saline 1 day before surgery. On the day of surgery, an incision was made for a midline laparotomy. Open surgery was preferred over laparoscopic or robotic techniques because it enables better bleeding control, safer dissection, and more dependable, thorough excision due to the tumor's hypervascular nature and proximity to major vessels.
The transverse colon and omentum were retracted cranially. The small bowel was retracted to the right side of the patient. The mass was identified (Fig. 3). We started by dissecting at the right side of the mass, just from the border of the anterolateral side of the infrarenal aorta, starting caudally and moving forward cranially all the way to the left renal vein. All the pedicles were double-tied and transected. There was a fluctuation in blood pressure. However, it did not exceed a systolic value of 190. After mobilizing the right side of the mass and attaching it to the abdominal aorta, we moved into the cranial side of the mass, dissecting it free from the left renal vein and from the gonadal as well as the posterior side of the mass until rebound hypotension was controlled with fluid and Levophed. Postoperatively, the patient was admitted to intensive care unit for monitoring. On postoperative day 1, the patient was off inotropes and Antihypertensive medications were stopped. Histopathology revealed a PGL with no lymphovascular invasion or capsular invasion. The patient was discharged home on postoperative day 3, with normal blood pressure readings, even in the long-term follow-ups in the clinic.
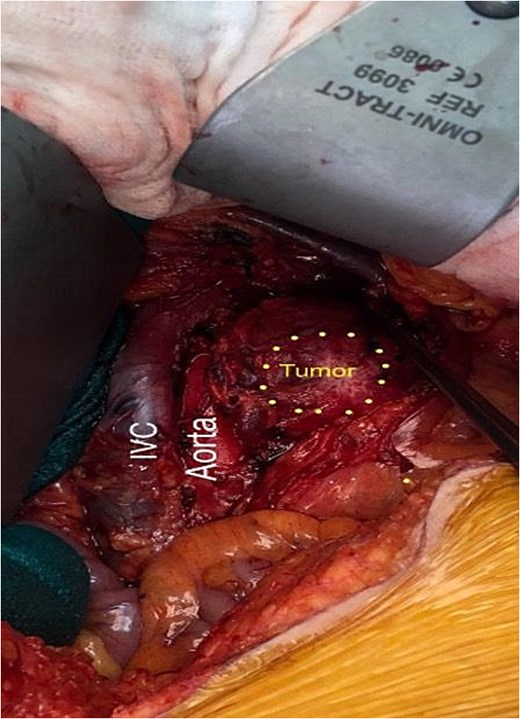
Retroperitoneal tumor adjacent to the aorta and inferior vena cava.
Discussion
Failure of three antihypertensive medications, including a diuretic, at optimal doses should raise the suspicion of secondary hypertension [4]. In the most recent guidelines for managing hypertension in patients with PGL in 2023, the experts recommended a multidrug, stepwise preoperative approach to prevent hypertension complications, starting by initiating alpha-adrenergic blockade for a period of 7–14 days before surgery. Moreover, beta-blockers used to treat tachycardia should not be administered before an appropriate and adequate alpha blockade is achieved to prevent hypertensive crisis [5]. The most common added-on drugs used concurrently with alpha blockers are calcium channel blockers [6]. A high-sodium diet with one to 2 l of normal saline is recommended 24 h before surgical resection to reduce the risk of hypotension [7].
In an update on modern management of PCC and PGL published by Lenders et al. [2], the imaging approach strategies prefer CT as the first modality because of its high spatial resolution for the thorax, abdomen, and pelvis, and high sensitivity for adrenal tumors of up to 90%, whereas it is less sensitive for metastatic or extramedullary tumors. MRI is preferred for skull base and neck PGLs, extra-adrenal PGLs, or those whose CT findings are contraindicated. The most frequently used functional imaging method is 123I-MIBG for scintigraphy and SPECT, which has a sensitivity for detecting adrenal PCCs of up to 100%, but it has a low percentage for extra-adrenal PGLs (56% to 75%) and metastases.
Author contributions
Khalid Alshehri (Data curation, Methodology, Writing—original draft, Writing—review & editing), Alwaleed Alsahafi (Data curation, Methodology, Writing—original draft), Haythem Alabbas (Conceptualization, Project administration, Supervision, and Validation), and Heitham Albeshri (Conceptualization, Project administration, Supervision, and Validation)
Conflicts of interest
The authors declare no competing interests.
Funding
This research didn’t receive any funding.
Data availability
All data generated or analyzed during this study are included in this published article.
Ethics approval statement
The authors confirm that the research meets the ethical standards set by relevant authorities, thereby protecting the rights of participants. Informed consent was obtained from the participant included in the study.

{kind=link}
{kind=link}
{kind=link}