





Abstract
Buschke–Lowenstein tumour (giant condyloma acuminatum) is a rare sexually transmitted lesion associated with human papillomavirus infection, most commonly types 6 and 11. Although histologically benign, it demonstrates locally aggressive growth, high recurrence rates, and potential malignant transformation. We report two cases of large circumferential Buschke–Lowenstein tumours involving the anorectal region. Both patients presented with progressively enlarging exophytic lesions requiring surgical management. Wide local excision was performed in both cases, followed by reconstruction with bilateral V-Y advancement flaps due to extensive tissue defects. Histopathological examination confirmed giant condyloma acuminatum without evidence of dysplasia or invasive carcinoma. Postoperative recovery was uneventful and no early recurrence was observed during follow-up. These cases highlight the importance of complete surgical excision with adequate margins and appropriate reconstructive techniques in the management of extensive perianal Buschke–Lowenstein tumours.
Introduction
Buschke–Lowenstein tumour is a rare, locally aggressive variant of giant condyloma acuminatum, first described by Buschke and Lowenstein in 1925 [1]. It is strongly associated with human papillomavirus infection, most commonly types 6 and 11. Although histologically benign, the tumour demonstrates progressive local growth, high recurrence rates, and a risk of malignant transformation [2]. Early diagnosis and prompt surgical management are critical to prevent extensive tissue damage and functional loss.
Case reports
Case 1
A 20-year-old man with a history of topical treatment for anal condylomas presented with months of perianal discomfort, intermittent bleeding, and progressive swelling. No systemic symptoms were reported. Examination revealed a large circumferential exophytic perianal lesion measuring ~10 × 10 cm involving the entire anal margin. The lesion appeared erythematous, friable, and bled on contact. Surrounding tissues were edematous. No inguinal lymphadenopathy or sphincter involvement was detected. HIV serology and syphilis testing were negative (Fig. 1). Wide local excision of the circumferential lesion was performed (Fig. 2). The tumour involved the anoderm without invasion of the deep sphincter. Primary closure was not possible due to the defect size, therefore reconstruction was performed using a V-Y advancement flap (Fig. 3). This technique mobilized well-vascularized tissue to cover the defect and preserve anal sphincter function (Fig. 4). Deep subcutaneous approximation was performed with absorbable sutures followed by interrupted skin sutures (Fig. 5). Histopathological examination demonstrated papillomatous squamous proliferation supported by fibrovascular cores. The epithelium showed acanthosis, parakeratosis, and koilocytic changes consistent with HPV infection. Resection margins were negative. No dysplasia or invasive carcinoma was identified. The postoperative course was uneventful. The patient was discharged on Day 5. At 8-month follow-up no recurrence was observed and anorectal function was preserved (Fig. 6).

Large circumferential exophytic Buschke–Lowenstein tumor involving the perianal region in Case 1.

Resected circumferential exophytic lesion following wide local excision in Case 1.
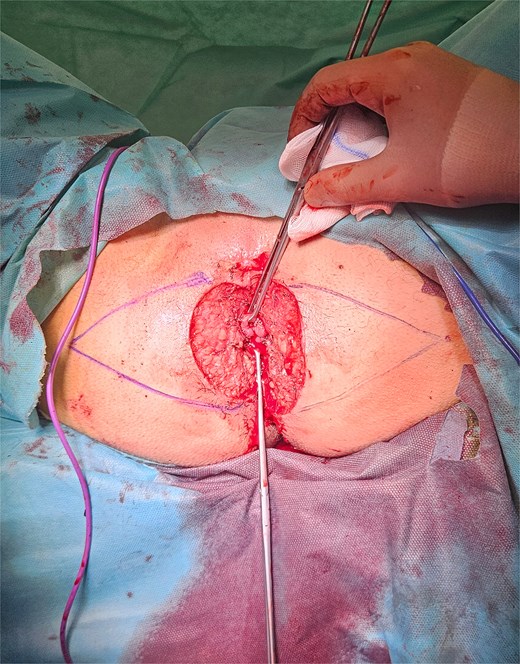
Intraoperative preparation for reconstruction with bilateral V-Y advancement flaps in Case 1.
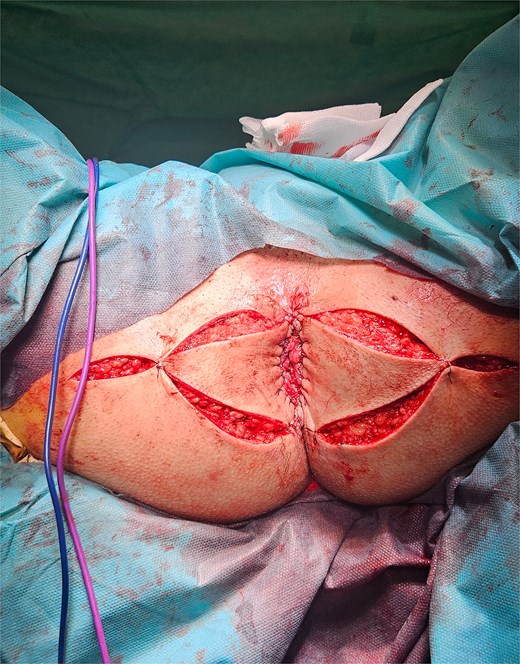
Tension-free closure and preservation of the anal sphincter region in Case 1.

Postoperative day 5 demonstrating viable bilateral V-Y advancement flaps and satisfactory wound healing in Case 1.

Late postoperative follow-up demonstrating well-healed bilateral V-Y advancement flaps without evidence of local recurrence in Case 1.
Case 2
A 32-year-old man presented with a 6-month history of progressively enlarging anal lesions and pain. Physical examination revealed a large circumferential exophytic anal condylomatous mass measuring ~7 × 9 cm involving the anal margin. No sphincter or deep tissue invasion was observed. HIV serology and syphilis testing were negative (Fig. 7).

Preoperative clinical presentation of a circumferential verrucous perianal mass consistent with Buschke–Lowenstein tumor in Case 2.
En bloc excision of the lesion was performed with removal to healthy tissue margins while preserving sphincter integrity. The defect was reconstructed using a V-Y advancement flap to achieve adequate coverage and reduce the risk of postoperative stenosis. Histological examination demonstrated papillomatous squamous hyperplasia supported by fibrovascular cores with hyperkeratosis, changes consistent with HPV infection. Resection margins were negative for dysplasia or invasive carcinoma. During the first postoperative month the patient experienced mild transient incontinence of flatus and liquid stool which resolved spontaneously. Endoscopic evaluation at two months revealed no additional lesions in the anal canal or colon. At 6-month follow-up no recurrence was observed and continence was fully restored (Fig. 8).

Late postoperative follow-up showing stable scar formation and preserved anal contour after bilateral V-Y advancement flap reconstruction in Case 2.
Discussion
Buschke–Lowenstein tumour is characterized by locally aggressive behavior despite benign histological features [1]. In a series of 42 patients, Chu et al. reported recurrence rates of ~66% and malignant transformation in up to 56% of cases [2]. These data underscore the need for complete surgical excision and vigilant follow-up.
Immunosuppression is an important risk factor for extensive disease and recurrence. García Cruz et al. reported successful surgical treatment of a Buschke–Lowenstein tumour in an HIV-positive patient using wide excision and V-Y advancement flap reconstruction [3]. Clinically, Buschke–Lowenstein tumour usually presents as a large exophytic verrucous mass in the anorectal region with progressive enlargement, ulceration, and bleeding [2]. Similar HPV-related lesions may occur at other cutaneous or mucosal sites [4].
Wide surgical excision with histologically negative margins remains the cornerstone of treatment [2, 5]. In extensive perineal lesions, primary closure is often not feasible and may predispose to wound complications or anal stenosis.
In a series of seven patients, all cases were treated with wide excision, with reconstruction adapted to defect size [6].
Ajagbe et al. reported three patients treated with wide excision, two requiring flap reconstruction, and one managed by secondary intention [7]. Similarly, García Cruz et al. demonstrated that V-Y advancement flap reconstruction can provide satisfactory healing and preservation of anal function even in complex cases [3].
Long-term outcomes following radical excision combined with flap reconstruction have also been reported. In a series of 11 patients undergoing wide local excision with flap coverage, no local recurrence, or anal stenosis was observed during a mean follow-up of over 50 months, suggesting that flap reconstruction may reduce the risks of relapse and postoperative stenotic complications [8].
Anal stenosis is one of the most significant functional complications following wide perianal excision. Mihailov et al. reported a case of extensive perianal Buschke–Lowenstein tumour treated with wide resection and V-Y flap reconstruction, in which postoperative anal stenosis required subsequent dilatation [9]. This finding highlights the importance of careful reconstructive planning and structured postoperative follow-up to preserve anorectal function.
Skowrońska-Piekarska and Kościński reported extensive perianal resection with immediate flap reconstruction without fecal diversion, demonstrating that a diverting stoma may be avoided in carefully selected patients when preoperative assessment excludes deep sphincter or visceral invasion and adequate wound protection is ensured [10].
In both patients described in this report, reconstruction was performed using a V-Y advancement flap. This technique provided reliable coverage of large perianal defects while preserving sphincter integrity and resulted in favourable early postoperative outcomes. No malignant transformation or recurrence was observed during initial follow-up. However, given the well-documented recurrence risk reported in larger series, [2] long-term surveillance remains essential.
Human papillomavirus infection plays a central role in the pathogenesis of Buschke–Lowenstein tumour. Viral oncogenes E6 and E7 inactivate tumour suppressor proteins such as p53 and retinoblastoma, promoting dysregulated cell proliferation and increasing the risk of malignant transformation [11, 12]. The main limitation of this report is the relatively short follow-up period. Buschke–Lowenstein tumour is rare but locally aggressive, necessitating early diagnosis, and radical surgical management. Wide excision with negative margins is essential. For large perineal defects, the V-Y advancement flap represents a reliable reconstructive option that provides adequate wound coverage and preserves anal function. Long-term follow-up is necessary due to the high risk of recurrence.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
The authors received no financial support for this study.
Patient consent
Written informed consent was obtained from the patients for publication of this case report and any accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}