





Abstract
Hepatic arterial variations are frequently encountered during hepatopancreatobiliary surgery; however, the majority conforms to established patterns described in classical classification systems. A replaced right hepatic artery most commonly arises from the superior mesenteric artery, while origin directly from the celiac trunk is exceptionally rare and not represented in standard classifications. We report a case of a replaced right hepatic artery arising directly from the celiac trunk encountered during pancreaticoduodenectomy in a patient with mixed-type intraductal papillary mucinous neoplasm complicated by acute cholangitis and prior endoscopic biliary stenting. Despite comprehensive preoperative cross-sectional imaging, the arterial anomaly was not identified and was recognized only during meticulous intraoperative dissection. A review of patient-based clinical literature identified four published case reports describing a total of five patients with a right hepatic artery arising directly from the celiac trunk. The present case represents an additional clinical example, further expanding the limited patient-based evidence.
Introduction
Anatomical variations of the hepatic arterial system are common and of critical importance in hepatopancreatobiliary surgery. Classical descriptions by Michels and subsequent simplification by Hiatt account for the majority of clinically encountered variants, particularly those involving replaced or accessory right hepatic arteries (RHA) arising from the superior mesenteric artery [1, 2].
The most common replaced RHA arises from the superior mesenteric artery (SMA) and is well recognized by both surgeons and radiologists [3]. In contrast, origin of an rRHA directly from the celiac trunk is exceedingly rare and sparsely documented in literature [4, 5]. This configuration is not included in standard hepatic arterial classification systems and is therefore prone to being overlooked, particularly during complex pancreatic surgery.
A literature search was conducted using PubMed, supplemented by targeted Google Scholar searches, to identify four patient-based clinical and imaging reports describing a right hepatic artery arising directly from the celiac trunk.
Four patient-based case reports describing a total of five patients with a right hepatic artery arising from the celiac trunk were identified in the peer-reviewed literature [4–7]. Cadaveric anatomical series and prevalence studies were excluded, as they do not provide direct clinical or operative context.
The report by Bastos-Neves et al. [7] describes an accessory right hepatic artery arising from the celiac trunk; however, this represents a supplementary vessel rather than a true replaced artery.
The literature demonstrates that this arterial configuration is exceedingly rare, with most large anatomical and radiological series reporting an incidence well below 1% or not identifying it at all [8]. Importantly, this variant is not included in the classical Michels or Hiatt classifications.
We present a case of this rare arterial variant encountered during pancreaticoduodenectomy for intraductal papillary mucinous neoplasm (IPMN) in a patient with antecedent acute cholangitis and biliary stenting, and provide a focused review of the existing patient-based literature.
Case description
A 38-year-old woman presented with recurrent right upper quadrant pain, progressive jaundice, and fever. She underwent endoscopic retrograde cholangiopancreatography with biliary stent placement, and was subsequently referred for definitive surgical management.
Contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatography demonstrated a bulky pancreatic head and uncinate process with clustered, thin-walled, intercommunicating cystic lesions communicating with a dilated main pancreatic duct, consistent with mixed-type intraductal papillary mucinous neoplasm. The lesion caused extrinsic compression and abrupt narrowing of the intrapancreatic common bile duct with upstream biliary dilatation. Major abdominal vessels were reported as grossly normal, and no aberrant hepatic arterial anatomy was identified preoperatively, likely influenced by inflammatory changes and the presence of a biliary stent (Fig. 1A–F).
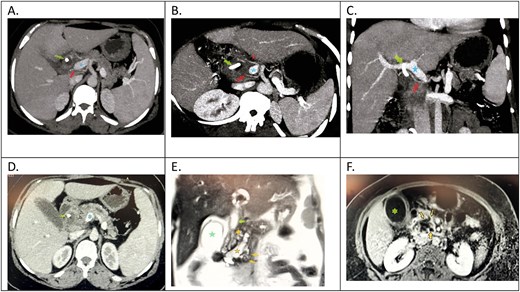
Contrast-enhanced CT and MRI findings. (A–D) Axial and coronal contrast-enhanced CT images demonstrating a replaced right hepatic artery (red arrow) arising directly from the celiac trunk, coursing posterior to the portal vein (blue star), and common bile duct with indwelling stent (green arrow). The common hepatic artery (red arrowhead) is seen originating separately from the celiac trunk. The pancreatic head mass causes compression at the portal vein–splenic vein confluence (black arrowheads).
(E and F) MRI images showing multiple dilated pancreatic side branches (gold arrowheads) communicating with a dilated main pancreatic duct (gold star), along with a distended gallbladder (green star) and dilated common bile duct (green arrow), consistent with mixed-type intraductal papillary mucinous neoplasm with biliary compression. The ampulla demonstrates a characteristic fish-mouth appearance (arrow).
At surgical exploration, a replaced right hepatic artery was identified arising directly from the celiac trunk, coursing posterior to the bile duct and portal vein before entering the liver parenchyma independently (Fig. 2A and B).
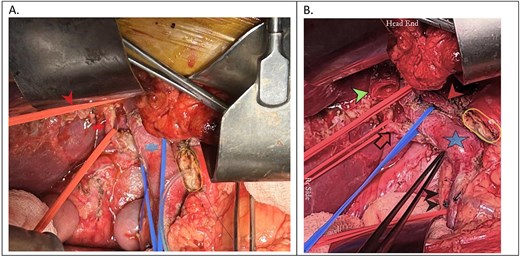
Intraoperative demonstration of hepatic arterial anatomy in the same patient. (A) A replaced right hepatic artery (red arrow) arising independently and coursing posterior to the portal vein (blue star), meticulously dissected and looped. The common hepatic artery (red arrowhead) is seen separately looped. The pancreatic cut surface following pancreatic transection is visible, with an infant feeding tube placed in the main pancreatic duct (golden oval). (B) The replaced right hepatic artery (red arrow) coursing posterior to both the portal vein (blue star) and common hepatic duct (green arrowhead), highlighting its close relationship to critical biliary structures. The superior mesenteric artery (black arrowhead) and hepatic artery proper (red arrowhead), both separately identified and looped, confirm that the right hepatic artery does not originate from the superior mesenteric artery.
The vessel was carefully dissected and preserved. A standard pancreaticoduodenectomy was completed without vascular injury. The postoperative course was uneventful, with preserved hepatic function and no biliary complications.
Final histopathology revealed a mixed-type intraductal papillary mucinous neoplasm of the pancreas with associated invasive adenocarcinoma, showing lymphovascular invasion, negative resection margins, and no lymph node metastasis (pT3N0, AJCC 8th edition).
Discussion
Hepatic arterial variations are reported in up to 40%–45% of individuals; however, most conform to patterns described by Michels or Hiatt [8]. In both systems, replaced or accessory right hepatic arteries are defined as arising from the SMA. A right hepatic artery originating directly from the celiac trunk is absent from these classifications and is typically categorized as an unclassified anomaly.
Large CT angiographic series further confirmed the extreme rarity of this variant. Choi et al. [9] identified only five cases of replaced or accessory RHA arising from the celiac trunk among 5625 patients evaluated, without individual clinical or intraoperative correlation.
After exclusion of cadaveric anatomical studies, a review of patient-based literature identified four published case reports describing a total of five patients with a right hepatic artery arising directly from the celiac trunk (Table 1) [4–7].
Patient-based reports of replaced and accessory right hepatic arteries arising from the celiac trunk (cadaveric studies excluded).
| Year | Author | No. of cases | Type of RHA from celiac trunk | Clinical / study context | Reference journal |
|---|---|---|---|---|---|
| 2016 | Katagiri H. et al. [6] | 1 | Replaced RHA from celiac trunk | Laparoscopic cholecystectomy – intraoperative pitfall | Asian J Endosc Surg. 2016;9:72–74 |
| 2016 | Bastos-Neves D. et al. [7] | 1 | Accessory RHA from celiac trunk | Living donor liver transplantation (donor anatomy) | Transplant Proc. 2016;48:2387–2388 |
| 2022 | Behera A. et al. [5] | 1 | Replaced RHA from celiac trunk | Pancreaticoduodenectomy – surgical relevance | Cureus. 2022;14:e21402 |
| 2024 | Osman B. et al. [4] | 2 | Replaced RHA from celiac trunk | CT angiography with intraoperative confirmation | Radiol Case Rep. 2025;20:449–453 |
| 2025 | Present case | 1 | Replaced RHA from celiac trunk | Difficult pancreaticoduodenectomy for IPMN after cholangitis | Present study |
Of these, four patients had a replaced RHA, while one had an accessory RHA. These cases were encountered during laparoscopic cholecystectomy, pancreaticoduodenectomy, liver transplantation, or cross-sectional imaging, underscoring the significant surgical relevance of this rare arterial variant. The present case represents an additional clinical example, further expanding the limited patient-based evidence.
The five cases reported by Choi et al. [9] were derived from a large CT angiographic prevalence study without detailed clinical presentation, operative findings, or surgical outcomes, and are therefore considered separately from patient-based clinical and surgical reports.
In the present case, the arterial anomaly was not detected on preoperative imaging. This is plausibly explained by the presence of acute cholangitis, periportal inflammation, and prior biliary stenting, all of which may obscure small or aberrantly coursing vessels and reduce the sensitivity of cross-sectional angiographic assessment.
From a surgical perspective, unrecognized injury to a replaced right hepatic artery during pancreaticoduodenectomy may result in hepatic ischemia, biliary anastomotic failure, liver abscess, or postoperative liver dysfunction—risks that are further amplified in inflamed operative fields.
Highlights
A replaced right hepatic artery arising directly from the celiac trunk is an exceptionally rare vascular variant and is not represented in standard hepatic arterial classification systems.
We report this variant encountered during a technically difficult pancreaticoduodenectomy for intraductal papillary mucinous neoplasm in a patient with prior acute cholangitis and biliary stenting.
Preoperative cross-sectional imaging failed to identify the aberrant artery, likely due to inflammatory changes and the presence of a biliary stent, underscoring limitations of imaging in such settings.
A focused review of patient-based literature identified only four published case reports describing five patients with this arterial configuration, highlighting its extreme rarity and surgical relevance.
Awareness of this uncommon arterial anatomy and meticulous intraoperative dissection are critical to prevent inadvertent vascular injury during complex hepatopancreatobiliary surgery.
Conflicts of interest
None declared.
Funding
None declared.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to patient confidentiality and institutional policies. However, de-identified data may be made available from the corresponding author upon reasonable request and with appropriate ethical and institutional approvals.

{kind=link}
{kind=link}