





Abstract
Hereditary protein S deficiency is a rare thrombotic disease caused by pathogenic variants in the PROS1 gene, predisposing individuals to an increased risk of venous thromboembolism. A 41-year-old male patient with a history of cerebral venous sinus thrombosis presented to the emergency department with acute abdominal pain and hematochezia. Contrast-enhanced computed tomography showed portal, splenic, and superior mesenteric venous thrombosis. Complicated by acute intestinal ischemia, the patient underwent emergency bowel resection. Laboratory assays demonstrated markedly reduced protein S activity. Next-generation sequencing identified a heterozygous deletion in the PROS1 gene, resulting in a frameshift mutation and the creation of a premature termination codon. To date, this variant has not been previously reported, representing a novel pathogenic mutation of the PROS1 gene. This case highlights the critical importance of investigating hereditary thrombophilia in young patients presenting with acute abdominal pain and unprovoked thrombosis at atypical sites, facilitating timely diagnosis and appropriate long-term management.
Introduction
Protein S is a vitamin K-dependent glycoprotein that plays a critical role in the anticoagulation system. Hereditary protein S deficiency (PSD) is an autosomal dominant thrombophilia caused by pathogenic variants in the PROS1 gene. These genetic alterations result in reduced protein S activity or levels, leading to impaired anticoagulant capacity and an increased risk of thrombosis [1, 2]. PSD is commonly associated with venous thromboembolism, particularly recurrent deep vein thrombosis and pulmonary embolism [3]. In rare cases, thrombosis may occur at atypical sites, such as the splanchnic veins, potentially resulting in acute intestinal ischemia, necrosis, or perforation [4–6].
Here, we report a case of extensive splanchnic venous thrombosis complicated by intestinal ischemic necrosis as the initial manifestation of a novel PROS1 gene mutation, successfully managed with emergency surgery and long-term anticoagulation.
Case presentation
A 41-year-old man presented to our emergency department in May 2025 with 2 days of mid-abdominal pain. The pain, initially intermittent and refractory to symptomatic treatment, progressed to persistent colic accompanied by hematochezia over the past 24 h. He had been diagnosed with cerebral venous sinus thrombosis (CVST) 13 years ago, and underwent anticoagulation therapy for 3 months without regular follow-up. Family history was negative for thrombotic diseases or malignant tumors.
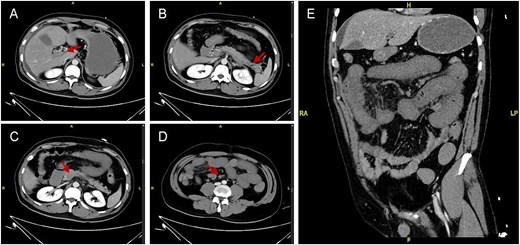
Representative contrast-enhanced abdominal CT images. (A) Formation of multiple collateral vessels around the main portal trunk. The portal vein (A; arrow), splenic vein (B; arrow), and superior mesenteric vein (C, D; arrows) showed an absence of contrast enhancement. (E) Extensive thickening and hypoenhancement of the small bowel wall, accompanied by surrounding mesenteric stranding.
On admission, his vital signs were stable. Abdominal examination revealed marked mid-abdominal tenderness and hypoactive bowel sounds, without rebound tenderness or abdominal guarding. Laboratory testing showed an arterial blood lactate level of 7.5 mmol/L, leukocytosis (20.44 × 109/L; 89.2% neutrophils), and a D-dimer level of 29.88 mg/L FEU (Table 1). Further evaluation with contrast-enhanced abdominal computed tomography (CT) suggested thrombosis of the portal (PV), splenic, and superior mesenteric veins. Diffuse small bowel wall thickening with hypoenhancement was observed, highly suggestive of ischemic necrosis (Fig. 1).
Routine test results.
| Test name | Case | Reference range | Test name | Case | Reference range |
|---|---|---|---|---|---|
| pH | 7.28 | 7.35–7.45 | Cl | 109 | 96–111 mmol/L |
| PaCO₂ | 31 | 35–45 mmHg | Ca | 2.21 | 2.11–2.52 mmol/L |
| PaO₂ | 86 | 83–108 mmHg | ALT | 80 | 9–50 U/L |
| HCO₃− | 14.4 | 22–27 mmol/L | AST | 37 | 15–40 U/L |
| LAC | 7.5 | 0.5–1.6 mmol/L | Alb | 36 | 35–52 g/L |
| WBC | 20.44 | 3.50–9.50 × 109/L | TBil | 68.1 | 5.1–22.2 μmol/L |
| RBC | 4.75 | 4.00–5.50 × 1012/L | DBil | 30.5 | ≤6.8 μmol/L |
| HGB | 148 | 120–160 g/L | Glu | 7.4 | 3.9–6.1 mmol/L |
| PLT | 190 | 100–350 × 109/L | BUN | 11.6 | 2.8–7.2 mmol/L |
| hsCRP | 123.70 | <3 mg/L | Cr | 103 | 59–104 μmol/L |
| PCT | 1.70 | <0.25 ng/ml | UA | 239 | 210–416 μmol/L |
| PT | 14.8 | 10.4–12.6 s | LDH | 243 | 0–250 U/L |
| INR | 1.30 | 0.86–1.14 | CK | 253 | 24–195 U/L |
| Fbg | 2.61 | 1.80–3.50 g/L | CK-MB | 1.4 | ≤5.0 μg/L |
| APTT | 25.3 | 23.3–32.5 s | Myo | 173 | ≤110 μg/L |
| TT | 16.1 | 14.0–21.0 s | hscTnI | 6 | ≤54 ng/L |
| D-Dimer | 29.88 | 0–0.55 mg/L FEU | NT-proBNP | 72 | 0–125 pg/ml |
| K | 3.7 | 3.5–5.5 mmol/L | AMY | 64 | 36–143 U/L |
| Na | 140 | 135–145 mmol/L | LIP | 48 | 2–53 U/L |
Abbreviations: LAC, lactate acid; WBC, white blood cell; RBC, red blood cell; HGB, hemoglobin; PLT, platelet; hsCRP, high sensitivity C-reactive protein; PCT, procalcitonin; PT, prothrombin time; INR, international normalized ratio; Fbg, fibrinogen; APTT, activated partial thromboplastin time; TT, thrombin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Alb, albumin; TBil, total bilirubin; DBil, direct bilirubin; Glu, glucose; BUN, blood urea nitrogen; Cr, creatinine; UA, uric acid; LDH, lactate dehydrogenase; CK, creatine kinase; Myo, myoglobin; hscTnI, high-sensitivity cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide; AMY, amylase; LIP, lipase.
Initial management included nil per os, fluid resuscitation, analgesia, and empiric antibiotics. Following rapid deterioration into septic shock requiring vasopressors, an emergency exploratory laparotomy was performed. Intraoperatively, massive sanguineous ascites and extensive small bowel necrosis with mesenteric cyanosis were noted. The necrotic bowel, extending from 15 cm distal to the ligament of Treitz to ~ 150 cm proximal to the ileocecal valve, was resected. A side-to-side anastomosis was performed between the proximal jejunal remnant and the distal ileal remnant, with a protective enterostomy created 10 cm distally to the anastomotic site.
Postoperative thrombophilia screening revealed markedly reduced protein C and protein S activities (Table 2). Repeat testing 1 week later confirmed persistently low protein S activity (24%). Next-generation sequencing (NGS) identified a novel heterozygous frameshift variant in the PROS1 gene (Fig. 2). This mutation leads to a single-nucleotide deletion at position 1334 in exon 12 (NM_000313.4, c.1334delG), causing a reading-frame shift, converting arginine at codon 445 to leucine and introducing a premature termination codon downstream (p.Arg445Leufs*2). Consequently, a definitive diagnosis of hereditary PSD was established.
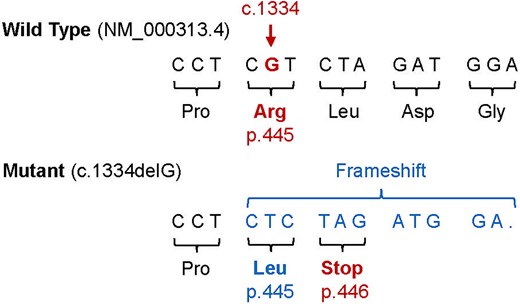
Schematic representation of the novel PROS1 gene mutation. The c.1334delG single-nucleotide deletion induces a frameshift, altering the amino acid at residue 445 from arginine (Arg) to leucine (Leu) and immediately creating a premature termination codon at position 446 (p.Arg445Leufs*2).
Thrombophilia-related test results.
| Test name | Case | Reference range | Test name | Case | Reference range |
|---|---|---|---|---|---|
| HCY | 6.8 | <15.0 μmol/L | aCL-IgG | 3.5 | <8.0 GPL U/ml |
| TG | 1.26 | <1.7 mmol/L | aCL-IgM | 2.0 | <8.0 MPL U/ml |
| TC | 1.81 | <5.2 mmol/L | aCL-IgA | <2.5 | <8.0 APL U/ml |
| HDL-C | 0.40 | >1.0 mmol/L | LA | 1.35 | ≤1.20 |
| LDL-C | 0.86 | <1.8 mmol/L | aPS/PT-IgG | <9.4 | ≤30.0 U |
| C3 | 0.847 | 0.730–1.460 g/L | p-ANCA | (−) | <1:10 |
| C4 | 0.215 | 0.100–0.400 g/L | c-ANCA | (−) | <1:10 |
| IgG | 7.09 | 7.00–17.00 g/L | Anti-PR3 | 2 | <16.0 AU/ml |
| IgA | 2.29 | 0.70–4.00 g/L | Anti-MPO | 1.8 | <16.0 AU/ml |
| IgM | 0.46 | 0.40–2.30 g/L | AFP | 1.2 | ≤20.0 ng/ml |
| ANA | (−) | <1:80 | CEA | 0.6 | ≤5.0 ng/ml |
| Anti-RNP | (−) | <10AI | CA19-9 | 2 | <34.0 U/ml |
| Anti-Sm | (−) | <10AI | CA72-4 | 0.9 | <9.8 U/ml |
| Anti-SSA | (−) | <10AI | CA125 | 5.4 | <35.0 U/ml |
| Anti-SSB | (−) | <10AI | CA242 | 2 | <25.0 U/ml |
| Anti-Scl-70 | (−) | <10AI | tPSA | 0.356 | ≤4.000 ng/ml |
| Anti-Ro52 | (−) | <10AI | fPSA | 0.131 | ≤0.930 ng/ml |
| Anti-dsDNA IgG | (−) | <1:10 | SCCAg | 0.7 | ≤2.7 ng/ml |
| Anti-β2-GP1 IgG | 4.2 | <16.0 AU/ml | NSE | 17.9 | ≤16.3 ng/ml |
| Anti-β2-GP1 IgM | <2 | <16.0 AU/ml | CYFRA21-1 | 1.7 | ≤3.5 ng/ml |
| Anti-β2-GP1 IgA | <2 | <16.0 AU/ml | ProGRP | 36.9 | ≤69.2 pg/ml |
| PS activity | 19 | 76%–135% | APC resistance | 2.3 | >2.1 |
| PC activity | 52 | 70%–140% | Antithrombin | 79 | 83%–128% |
Abbreviations: HCY, homocysteine; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; C3/C4, complement components 3 and 4; ANA, antinuclear antibody; Anti-RNP, anti-ribonucleoprotein antibody; Anti-Sm, anti-Smith antibody; Anti-SSA, anti-SSA antibody; Anti-SSB, anti-SSB antibody; Anti-Scl-70, anti-Scl-70 antibody; Anti-Ro52, anti-Ro52 antibody; Anti-dsDNA, anti–double-stranded DNA antibody; Anti-β2-GP1, anti-β2 glycoprotein 1 antibody; aCL, anti-cardiolipin antibody; LA, lupus anticoagulant; aPS/PT-IgG, anti-phosphatidylserine/prothrombin IgG; p-ANCA, perinuclear anti-neutrophil cytoplasmic antibody; c-ANCA, cytoplasmic anti-neutrophil cytoplasmic antibody; Anti-PR3, anti-proteinase 3 antibody; Anti-MPO, anti-myeloperoxidase antibody; AFP, alpha-fetoprotein; CEA, carcinoembryonic antigen; CA, carbohydrate antigen; tPSA, total prostate-specific antigen; fPSA, free prostate-specific antigen; SCCAg, squamous cell carcinoma antigen; NSE, neuron-specific enolase; CYFRA21-1, cytokeratin 19 fragment; ProGRP, pro-gastrin-releasing peptide.
The patient was bridged from continuous intravenous unfractionated heparin to subcutaneous low-molecular-weight heparin at discharge (postoperative Day 14). One month postoperatively, he was transitioned to oral rivaroxaban for lifelong anticoagulation. He remains under regular follow-up with no recurrence of thrombotic events reported to date.
Discussion
Portomesenteric venous thrombosis (PMVT) is a relatively uncommon but potentially life-threatening disease, accounting for ~ 5%–15% of mesenteric ischemia cases. Nonspecific early symptoms of PMVT frequently delay diagnosis and treatment, risking intestinal necrosis, perforation, and septic shock [7, 8]. In recent years, advanced imaging modalities like contrast-enhanced CT have improved the early detection and timely therapeutic intervention [9].
The etiology of venous thromboembolism (VTE) is generally categorized into acquired (such as malignancy, surgery, and pregnancy) and hereditary factors (such as factor V Leiden mutation, prothrombin G20210A mutation, and deficiencies of protein C/protein S/antithrombin) [8]. Hereditary PSD has an estimated prevalence of 0.16%–0.21% in the general population, yet it accounts for a significant proportion of unprovoked thrombotic events [1, 2, 10, 11]. This patient lacked clear acquired triggers but had a history of CVST, and subsequent laboratory testing revealed persistently low protein S activity, providing the pivotal clue for the diagnosis of hereditary thrombophilia. Protein S is encoded by the PROS1 gene. To date, over 200 mutations in the PROS1 gene have been reported, including missense, nonsense, and frameshift mutations caused by small deletions or insertions [1, 2, 10–12]. In this case, NGS analysis identified a heterozygous frameshift mutation in the PROS1 gene. This variant causes an amino acid substitution and the creation of a premature termination codon, which fulfills the PVS1 criterion of the American College of Medical Genetics and Genomics, classifying it as a novel pathogenic mutation. Accurately phenotyping PSD (types I, II, and III) requires integrating free protein S antigen levels, functional activity, and genetic analysis [13]. Due to the limited detection conditions, this patient failed to classify the specific deficiency phenotype. In addition, family genetic screening was not performed due to the family's financial constraints. These limitations highlight the real-world challenges of implementing standardized thrombophilia evaluation.
Anticoagulation remains the cornerstone of management for VTE. While there are no specific guidelines dedicated to hereditary PSD, management generally follows standard VTE principles, tailored to the patient's thrombotic phenotype and recurrence risk [8]. For acute PMVT, early anticoagulation is typically first-line to prevent thrombus extension and promote vessel recanalization. Surgical intervention is indicated only in cases with bowel necrosis, perforation, or clinical deterioration despite optimal conservative therapy [4–7, 14]. Given the unprovoked atypical thrombosis, massive thrombotic burden and confirmed pathogenic mutation, this patient was stratified as being at remarkably high-risk for thrombosis recurrence. Therefore, an indefinite (lifelong) anticoagulation strategy was recommended.
Conclusion
This case report describes a young male with extensive splanchnic venous thrombosis complicated by acute intestinal ischemia, ultimately diagnosed with hereditary PSD driven by a novel PROS1 gene mutation. This case highlights the critical importance of investigating hereditary thrombophilia in young patients presenting with unprovoked thrombosis at atypical sites. Prompt genetic identification and tailored, lifelong anticoagulation are vital to optimize outcomes and prevent catastrophic recurrence.
Acknowledgements
The authors gratefully acknowledge the contribution of the patient and hospital staff.
Author contributions
Jianlu Song collected the data and drafted this case report. Lizhen Qiu performed genetic analysis. All the authors reviewed the manuscript.
Conflicts of interest
The authors declared no potential conflicts of interest.
Funding
This study was supported by the National Natural Science Foundation of China (82403123), the fellowship of China Postdoctoral Science Foundation (2024T170074, 2024M760266, and GZB20240075).
Data availability
The data supporting this case report are available from the corresponding author upon reasonable request.
Ethical approval and informed consent
Ethical approval was obtained from the ethical committee of Peking Union Medical College Hospital. Written informed consent was obtained from the patient for publication of this case report.

{kind=link}
{kind=link}