





Abstract
Postoperative pancreatic fistula (PF) remains a serious complication after distal pancreatectomy (DP), particularly when it is refractory to standard management. Herein, we report a case of refractory Grade C PF following DP for pancreatic adenosquamous carcinoma. Despite conservative treatment, repeated image-guided percutaneous drainage, and endoscopic pancreatic duct stenting, the fistula persisted and was complicated by gastroduodenal artery bleeding and duodenal perforation. Given the patient’s early postoperative recurrence, poor prognosis, and high surgical risk, further surgical intervention was considered inappropriate. Pancreatic duct stump embolization using N-butyl-2-cyanoacrylate and vascular embolization coils was performed via a pull-through technique connecting the papilla of Vater to the percutaneous drainage route, resulting in successful closure of both the pancreatic duct and duodenal fistula. In selected patients with refractory PF, this approach may serve as a salvage treatment option when conventional therapies have failed or are overwise inappropriate.
Introduction
Postoperative pancreatic fistula (PF) is a serious complication after distal pancreatectomy (DP). Most cases can be managed conservatively, including drainage; however, some cases are refractory and difficult to manage. Here, we report a case of refractory PF involving the main pancreatic duct after DP for adenosquamous carcinoma (ASC) of the pancreatic body that was successfully managed with pancreatic duct embolization using N-butyl-2-cyanoacrylate (NBCA) and vascular embolization coils via a pull-through technique.
Case report
A 52-year-old man underwent DP with D2 lymphadenectomy and splenectomy for stage IIB pancreatic cancer (cT3N1aM0) according to the Union for International Cancer Control (UICC) 8th edition classification. The pancreatic stump was closed using the fish-mouth technique. Intraoperatively, tumor progression compared with the preoperative assessment was observed, and portal vein resection involving approximately two-thirds of the circumference was performed. A surgical drain was placed near the pancreatic stump. Postoperative pathological examination revealed pancreatic ASC, staged as pT4N1aM0 stage IIB (UICC 8th edition).
The patient’s postoperative clinical course is illustrated in Fig. 1. On postoperative day (POD) 3, the patient developed postoperative PF, and contrast-enhanced computed tomography (CT) revealed a fluid collection around the pancreatic stump (Fig. 2). Despite conservative management, including bowel rest, octreotide administration, and repeated image-guided percutaneous drainage with drain replacement and position adjustment, pancreatic juice leakage had persisted. On POD 17, endoscopic retrograde cholangiopancreatography (ERCP) revealed leakage from the main pancreatic duct, and a 5-Fr, 3-cm pancreatic duct stent (Geenen® Pancreatic Stent; Cook Medical, Tokyo, Japan) was placed. However, adequate fistula control was not achieved. The postoperative course was further complicated by bleeding from the gastroduodenal artery (GDA), which was successfully treated with transcatheter arterial embolization. Subsequently, duodenal perforation adjacent to the PF was identified. Endoscopic clip closure was performed; however, subsequent imaging demonstrated incomplete closure with persistent leakage (Fig. 3a–c).
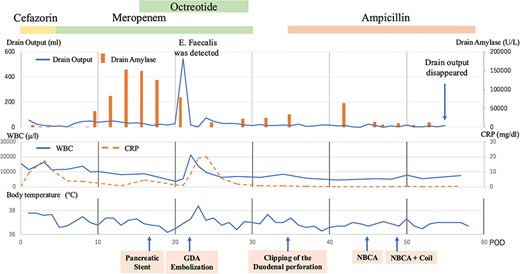
The patient’s clinical course after surgery.
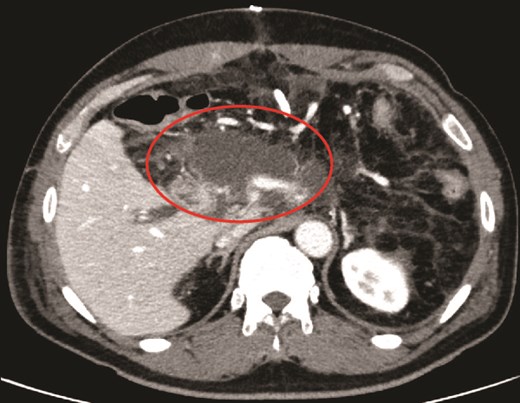
Contrast-enhanced CT revealed fluid collection around the pancreatic stump.
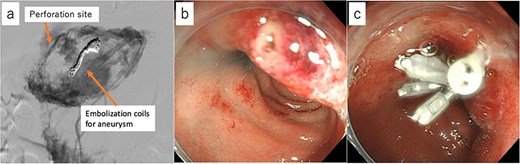
(a) Fluoroscopic imaging of the fluid-filled cavity revealed extravasation of contrast medium into the duodenum. (b) Endoscopic view showing the site of perforation in the duodenal bulb. (c) The perforation was closed with an endoscopic clip.
On POD 28, contrast-enhanced CT revealed a suspected metastatic liver lesion. Given the refractory nature of the PF, the presence of life-threatening complications, the patient’s early postoperative recurrence with poor prognosis, and his strong desire for early discharge, additional treatment options were carefully considered. Surgical reintervention was deemed inappropriate because of the high perioperative risk, and the pancreatic duct was identified as the source of leakage. Therefore, pancreatic duct stump embolization was selected as a salvage treatment option. On POD 45, endoscopic pancreatic duct stump embolization using NBCA mixed with lipiodol was performed under ERCP guidance. Multiple injections (0.5 ml each) were administered; however, the procedure was interrupted because of catheter occlusion, making endoscopic embolization alone technically challenging.
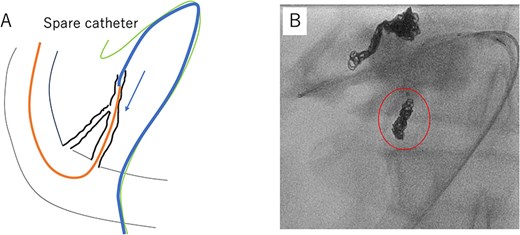
On POD 49, embolization was performed again. A pull-through technique was used to connect the papilla of Vater with the percutaneous drainage route, thereby enabling catheter manipulation from the percutaneous drain side. A guidewire introduced through the papilla of Vater was captured and externalized via the percutaneous drain site using a 10-mm Goose Neck™ snare (Medtronic, Tokyo, Japan), thereby establishing a through-and-through catheter access from the papilla of Vater to the percutaneous drain site (Fig. 4a and b). Vascular embolization coils (Target 3D Detachable Coils, Stryker) were deployed into the pancreatic duct stump, followed by NBCA injection (Fig. 5a and b). Embolization was also performed at the duodenal fistula site using coils and NBCA. After the procedure, pancreatic juice leakage had resolved, and imaging confirmed closure of both the pancreatic duct and duodenal fistula.
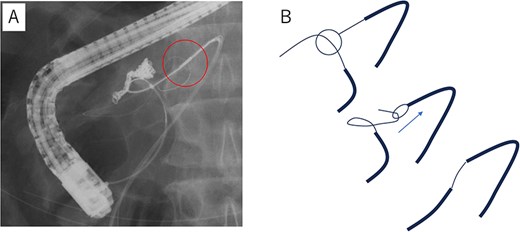
(a) A guidewire inserted through the endoscope from the papilla of Vater was caught and by a goose neck™ SNARE guided from the drain side and withdrawn through the drain insertion site. (b) Schematic illustration of the pull-through technique.
(a) The micro catheter was guided into the pancreatic duct through the percutaneous drain site over a guidewire. (b) Vascular embolization coils were placed in the pancreatic duct stump, followed by the injection of NBCA mixed with lipiodol into the coil deployment site.
The patient was discharged without recurrence of fistula-related complications. During follow-up, no symptoms suggestive of pancreatic exocrine or endocrine insufficiency were observed. He later received chemotherapy; however, no therapeutic response was observed, and he died of disease progression on POD 197.
Discussion
Postoperative PF is a challenging complication after DP, particularly when complicated by infection or hemorrhage. Conservative management, including drainage, bowel rest, somatostatin analogs, and nutritional support, is generally effective; however, some patients become refractory and require alternative interventions [1, 2]. In this case, standard treatment options were carefully considered and implemented sequentially. Repeated image-guided percutaneous drainage was performed through an indwelling surgical drain, and appropriate drainage of the abscess cavity was confirmed; however, fistula closure was not achieved. The clinical course was further complicated by GDA bleeding and duodenal perforation, prompting the consideration of a more definitive salvage strategy. Given the early postoperative recurrence of pancreatic ASC, a particularly poor-prognosis subtype [3, 4], and the patient’s strong desire for early discharge, surgical reintervention was considered but deemed inappropriate because of the high perioperative risk.
Embolization using materials such as NBCA mixed with lipiodol has been reported as a salvage approach for refractory PF, although clinical experience remains limited [5–8]. In the present case, endoscopic embolization alone was technically challenging because of catheter instability and early occlusion. To overcome these limitations, a pull-through technique combined with vascular embolization coils was employed. Pull-through technique is commonly used for catheter guidance in interventional radiology, particularly in vascular catheter procedures [9, 10]. This technique enabled a secure connection between the papilla of Vater and the percutaneous drainage route, allowing reliable catheter manipulation from the percutaneous side and precise delivery of embolic materials. Vascular embolization coils, although typically used for hemostasis [11], have reported the efficacy in treating biliary leaks [12, 13] and PF [14, 15]. Using vascular embolization coils provided mechanical anchoring and reduced the risk of NBCA migration, thereby facilitating effective embolization of the pancreatic duct stump.
Potential risks of pancreatic duct embolization include infection and pancreatic exocrine insufficiency; therefore, active intra-abdominal infection or uncontrolled abscess formation should be considered contraindications. In this case, no clinically significant exocrine or endocrine dysfunction was observed after discharge, and subsequent clinical deterioration was solely attributable to cancer progression.
In summary, pancreatic duct stump embolization using NBCA and vascular embolization coils via a pull-through technique may represent a feasible salvage option in highly selected patients with refractory PF when conventional therapies have failed or are otherwise inappropriate.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of interest
The other authors declare no conflicts of interest.
Funding
All authors have disclosed no financial relationships relevant to this publication.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}