





Abstract
Elastofibroma dorsi is a rare, benign pseudotumoral lesion of connective tissue that typically arises in the infrascapular region of elderly individuals. Due to its deep location and firm consistency, it may clinically and radiologically mimic malignant soft-tissue tumors, potentially leading to unnecessary biopsies or overtreatment. Characteristic imaging features, particularly on magnetic resonance imaging, usually allow a confident diagnosis. We report a case of right-sided elastofibroma dorsi in a 68-year-old male, describing the clinical presentation, imaging characteristics, surgical management, and histopathological findings. Additionally, a review of previously reported cases is presented, highlighting key learning points and diagnostic challenges.
Introduction
Elastofibroma dorsi is an uncommon benign connective tissue lesion, first described by Järvi and Saxén in 1961 [1]. It is classically located between the inferior angle of the scapula and the posterior thoracic wall, deep to the serratus anterior and latissimus dorsi muscles. Although considered rare, its true prevalence is likely underestimated, with autopsy studies reporting rates as high as 13%–24% in elderly populations [2].
The lesion predominantly affects older adults, with a slight female predominance, and is associated with repetitive mechanical friction between the scapula and chest wall [3]. Clinically, elastofibroma dorsi may be asymptomatic or present as a slowly growing mass with discomfort or restricted shoulder movement. Recognition of characteristic clinical and radiological features is essential to avoid unnecessary invasive diagnostic procedures.
We report a symptomatic case of elastofibroma dorsi managed surgically, followed by a concise literature review.
Case report
Case presentation
A 68-year-old male presented with a 1-week history of a gradually noticed mass in the right subscapular region. He reported mild local discomfort, particularly during shoulder movement, but denied pain at rest, skin changes, constitutional symptoms, or trauma.
On physical examination, a firm, mobile, well-circumscribed mass measuring ~10 cm was palpated in the right infrascapular area, becoming more prominent during shoulder abduction (Fig. 1). No overlying skin abnormalities or regional lymphadenopathy were observed, and systemic examination was unremarkable.

Firm, mobile, well-circumscribed 10 cm mass in the right infrascapular region, more prominent on shoulder abduction; overlying skin normal.
Radiological evaluation
Ultrasonography revealed a heterogeneous, hypovascular soft-tissue lesion in the subcutaneous and submuscular planes overlying the ribs, measuring 10 × 5 × 4 cm. Gray-scale imaging demonstrated a poorly circumscribed fibrofatty mass with alternating echogenic and hypoechoic linear areas (Fig. 2), and color Doppler showed minimal internal vascularity, suggesting a benign lesion (Fig. 3).
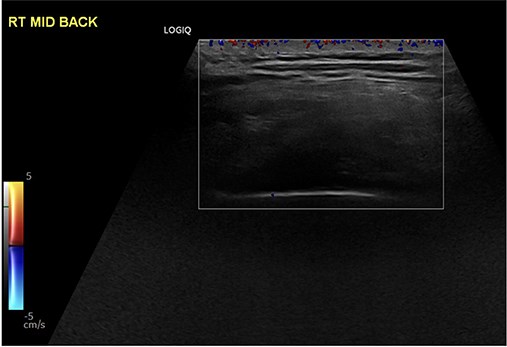
Gray-scale ultrasonography of the right subscapular region demonstrating a heterogeneous, poorly circumscribed soft-tissue mass with alternating hyperechoic and hypoechoic linear areas, consistent with a fibrofatty lesion.
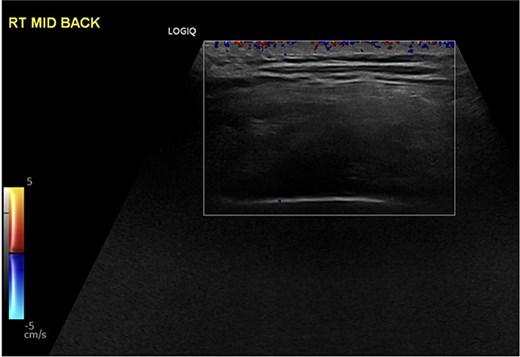
Color Doppler ultrasonography showing minimal internal vascularity within the right subscapular mass, supporting a benign etiology.
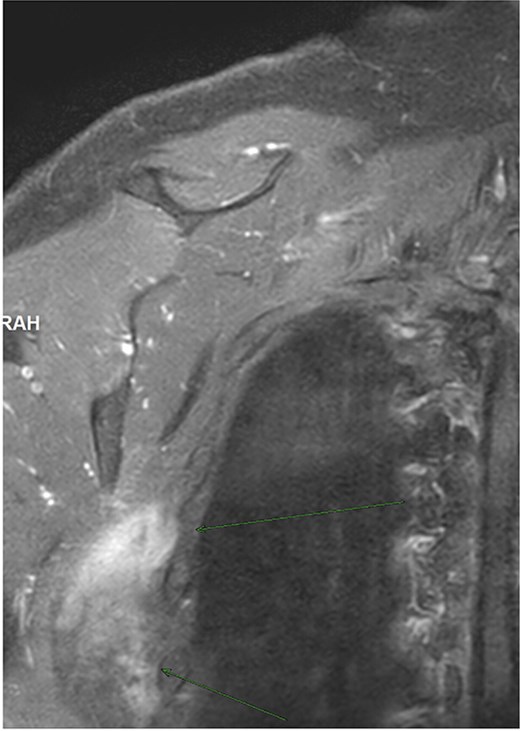
Magnetic resonance imaging (MRI) further characterized a poorly circumscribed mass at the posterolateral chest wall, just inferior to the scapula’s inferior angle, measuring 6.4 × 3.0 × 9.1 cm. The lesion displayed a striated ‘feathery’ appearance with alternating fibrous and fatty streaks, low to intermediate signal on T1- and T2-weighted images, and mild heterogeneous contrast enhancement (Figs 4 and 5). Coronal views delineated the craniocaudal extent of the mass between the scapula and chest wall, with preservation of adjacent structures and no aggressive features (Fig. 6). These imaging features—location, morphology, signal characteristics, and mild enhancement—were characteristic of elastofibroma dorsi [4].
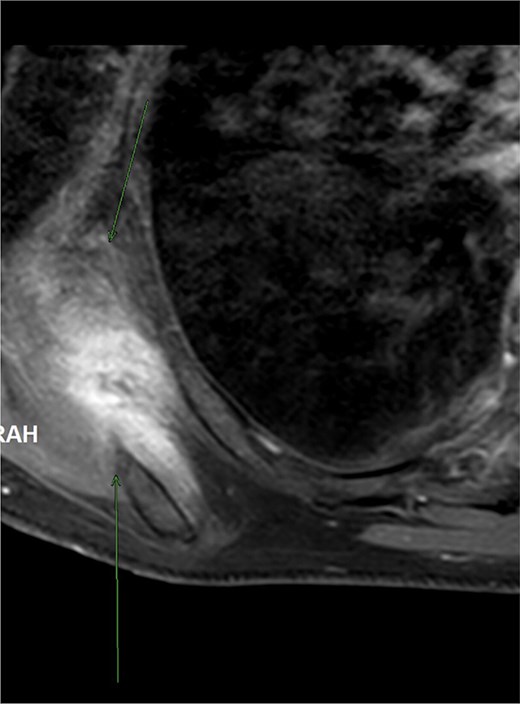
Axial T2-weighted fat-suppressed MRI demonstrating a poorly circumscribed mass in the right infrascapular region with a striated appearance due to alternating fibrous and fatty components.
Contrast-enhanced axial MRI showing mild heterogeneous enhancement of the right subscapular lesion without aggressive features, consistent with elastofibroma dorsi.
Contrast-enhanced coronal MRI demonstrating the craniocaudal extent of the right infrascapular mass located between the scapula and chest wall, with preservation of adjacent structures.
Surgical management
Given the patient’s symptoms and lesion size, elective surgical excision was performed. Under general anesthesia, a right infrascapular incision was made. Intraoperatively, a firm, oval, unencapsulated mass measuring ~7 cm was identified deep to the scapula, surrounded by the subscapularis, latissimus dorsi, and serratus anterior muscles, in direct contact with the rib cage (Fig. 7).
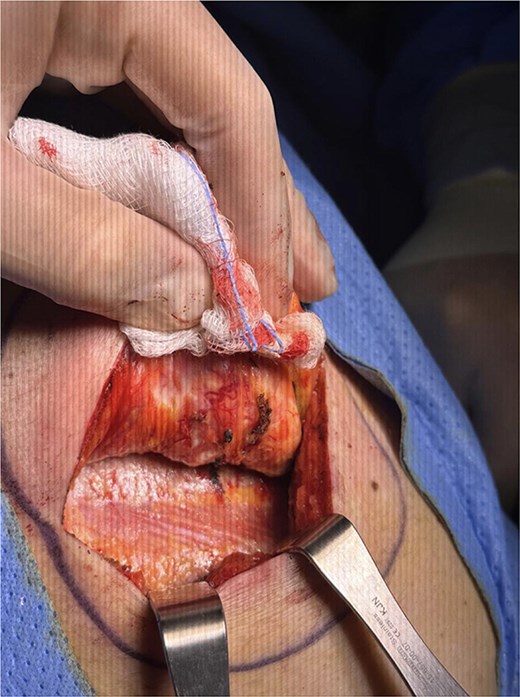
Intraoperative appearance of a firm, oval, unencapsulated 7 cm mass deep to the scapula, surrounded by subscapularis, latissimus dorsi, and serratus anterior muscles, in direct contact with the rib cage.
A marginal excision was completed, ensuring removal with surrounding healthy tissue. Hemostasis was achieved, and the wound was closed in layers. The postoperative course was uneventful, and the patient was discharged without complications.
Histopathological findings
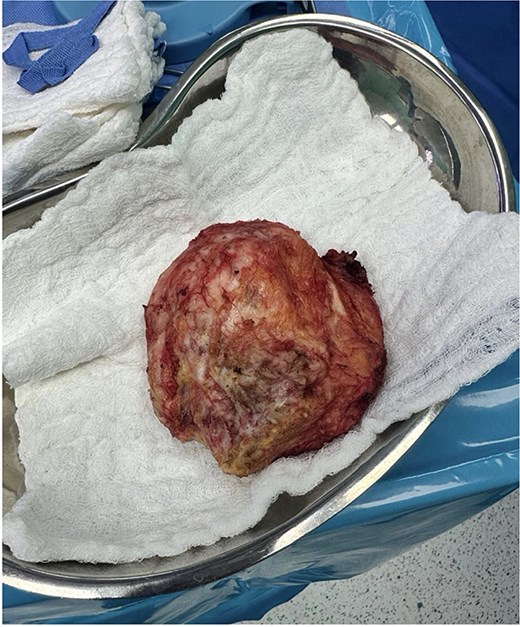
Specimen: Right subscapular mass, resection. Gross examination: The specimen measured 10.0 × 9.0 × 3.0 cm. The cut surface was heterogeneous, with alternating yellow (fatty) and white (fibrous) areas (Fig. 8).
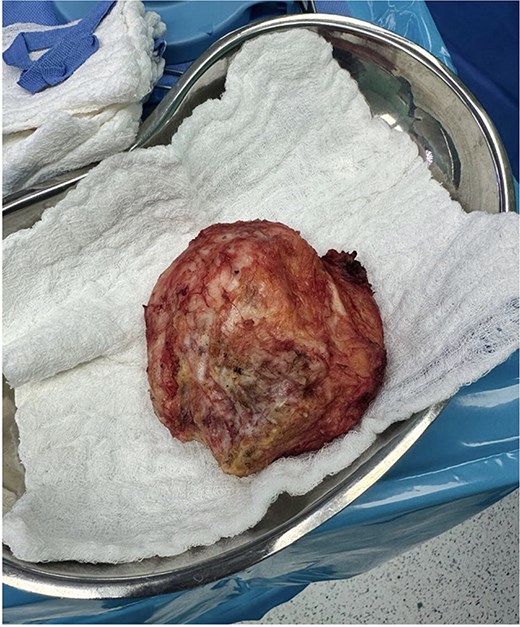
Gross pathological specimen of the resected right subscapular mass showing an unencapsulated lesion with a heterogeneous cut surface composed of alternating yellow (fatty) and white (fibrous) areas.
Microscopic examination: Histology revealed alternating bands of dense collagenous tissue containing abnormal, coarse elastic fibers interspersed with mature adipose tissue. No cellular atypia, mitotic activity, or necrosis was observed. Findings were diagnostic of elastofibroma dorsi (Fig. 9) [5].
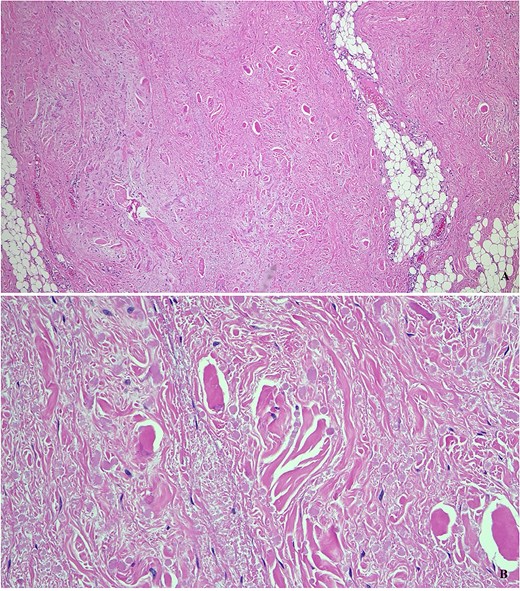
Histopathological examination (hematoxylin and eosin stain) revealing dense collagenous tissue containing abnormal elastic fibers interspersed with mature adipose tissue, confirming the diagnosis of elastofibroma dorsi.
Discussion
Elastofibroma dorsi is a benign pseudotumoral lesion, characterized by proliferation of abnormal elastic fibers within collagenous tissue and fat [1, 5]. Although fewer than 330 cases had been reported by the early 2000s, autopsy and imaging studies suggest the condition is more common than clinically recognized [2].
Clinically, it often presents as a deep infrascapular mass that becomes more prominent with shoulder movement. While many patients remain asymptomatic, discomfort, pain, or mechanical limitation may prompt evaluation [3]. Differential diagnoses include soft-tissue sarcoma, lipoma, desmoid tumor, and metastasis.
Imaging is pivotal. Ultrasonography typically shows a poorly circumscribed, layered or fasciculated lesion. MRI, the modality of choice, demonstrates alternating fibrous and fatty components with a pathognomonic ‘striated’ or ‘feathery’ pattern [4]. Typical imaging findings can establish diagnosis and avoid biopsy.
Surgical excision is indicated for symptomatic lesions, functional impairment, cosmetic concerns, or diagnostic uncertainty. Complete resection is recommended due to the absence of a true capsule; recurrence is rare and usually associated with incomplete excision [6]. Radiotherapy or chemotherapy has no role in management. Table 1 summarizes selected reported cases of elastofibroma dorsi, highlighting patient demographics, clinical presentation, management strategies, key learning points, and associated diagnostic or therapeutic challenges [1, 6–14].
Selected reported cases of elastofibroma dorsi with key learning points.
| Author / Year | Age / Sex | Side | Presentation | Management | Learning Points | Challenges |
|---|---|---|---|---|---|---|
| Järvi & Saxén, 1961 [1] | 60s / Female | Bilateral | Incidental finding | Surgical excision | First description; benign nature | Differentiation from malignancy |
| Nishida et al., 2012 [6] | 70s / Male | Unilateral | Pain with movement | Surgical excision | Excellent surgical outcomes reported | Risk of incomplete excision |
| Camara et al., 2025 [7] | 53 / Female | Bilateral (MRI diagnosis) | Slow, painless infrascapular swelling | Conservative management | MRI can avoid biopsy | Avoid unnecessary procedures |
| Köksel et al., 2005 [8] | 35 / Female | Left | Pain and swelling with shoulder movement | Surgical excision | Symptomatic lesions require surgery | Mimics soft-tissue tumor |
| Ohtake et al., 1998 [9] | 56 / Male | Left | Subscapular mass | Surgical excision | Consider in elderly patients with subscapular masses | Rare dermatologic presentation |
| Mortman et al., 2007 [10] | Case series | Mixed | Enlarging mass | Surgical resection | Surgery indicated when malignancy cannot be excluded | Diagnostic uncertainty |
| Saavedra et al., 2018 [11] | 85 / Male | Bilateral | Shoulder pain and limited range of motion | Rehabilitation | Can be managed conservatively | Rare cause of shoulder pain |
| Asaad et al., 2024 [12] | 51 / Female | Bilateral | Pain and activity limitation | Surgical excision | Symptomatic bilateral disease may require surgery | Functional impairment |
| Karti et al., 2022 [13] | Elderly / Female predominance | Bilateral (three cases) | Scapular masses | Surgical excision | Commonly bilateral in elderly women | Diagnosis and management considerations |
| Muratori et al., 2008 [14] | Mean age 70 / Female | 10% bilateral | Often incidental | Surgery if symptomatic | Follow-up acceptable if asymptomatic | Establishing management algorithm |
| Present case | 68 / Male | Right | Discomfort and palpable mass | Surgical excision | Imaging-guided diagnosis | Distinguishing from sarcoma |
Conclusion
Elastofibroma dorsi is a benign soft-tissue pseudotumor with characteristic clinical and radiological features. Awareness of this entity prevents unnecessary biopsies and overtreatment. MRI is usually sufficient for diagnosis, and surgical excision should be reserved for symptomatic or atypical lesions, with excellent outcomes and very low recurrence rates.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}