





Abstract
Tuberculous appendicitis is a rare form of extra-pulmonary tuberculosis that commonly mimics acute appendicitis and is usually diagnosed only after histopathological examination. A 35-year-old man presented with a 1-year history of intermittent abdominal pain and mucoid diarrhea before developing acute right lower quadrant pain due to perforated appendicitis requiring emergency appendectomy. Histopathology revealed caseating granulomatous inflammation consistent with tuberculous appendicitis. The patient completed 6 months of standard anti-tubercular therapy with complete resolution of symptoms. Due to its nonspecific clinical and radiologic presentation, tuberculous appendicitis is rarely diagnosed preoperatively. Routine histopathological examination of appendectomy specimens remains essential for diagnosis. Combined surgical and medical management typically results in an excellent prognosis.
Introduction
Tuberculosis (TB) remains a major global health problem, with extrapulmonary disease accounting for a significant proportion of cases [1]. Abdominal tuberculosis represents ~1%–3% of all TB cases and may involve the peritoneum, lymph nodes, or gastrointestinal tract [2, 3]. Within the gastrointestinal tract, the ileocecal region is most commonly affected, accounting for nearly 75% of intestinal TB cases [4, 5]. In contrast, isolated appendiceal involvement is exceedingly rare, reported in only 0.1%–0.6% of gastrointestinal tuberculosis [3, 5].
Tuberculous appendicitis may result from contiguous spread from ileocecal disease or, less commonly, occur as an isolated primary infection [5, 6]. Its presentation closely mimics acute appendicitis, and systemic features such as fever or weight loss are often absent, leading to low preoperative suspicion [7]. Laboratory and imaging findings are nonspecific and cannot reliably distinguish it from pyogenic appendicitis [7, 8]. Definitive diagnosis therefore relies on histopathological examination demonstrating caseating granulomas [7, 9]. For this reason, routine histopathological examination of all appendectomy specimens is recommended [9, 10].
Management consists of appendectomy followed by standard anti-tubercular therapy [11]. This combined approach has demonstrated excellent outcomes, with a recent review reporting cure in all cases treated with World Health Organisation (WHO)-recommended 6-month regimens [7]. We present a case of tuberculous appendicitis with an atypical chronic presentation and sequential ultrasonographic evolution highlighting the diagnostic challenges.
Case report
A 35-year-old man presented with a 1-year history of intermittent mucoid diarrhea associated with lower abdominal pain and tenesmus. Episodes lasted ~5 days and improved transiently with metronidazole. He denied fever, weight loss, anorexia, or night sweats. There was no history of TB treatment or contact. Also, he had no history of work-up or treatment for an inflammatory bowel disease.
On initial evaluation, vital signs were normal and abdominal examination was unremarkable. Laboratory investigations, including complete blood count, were within normal limits. Stool microscopy and fecal occult blood testing were negative. Ultrasonography demonstrated circumferential thickening of the cecum and appendix with enlarged mesenteric lymph nodes. A provisional diagnosis of irritable bowel syndrome was made, with inflammatory bowel disease considered.
During a subsequent episode, ultrasonography revealed a thickened but compressible appendix measuring 9 mm, with preserved wall stratification and minimal fat stranding, suggestive of chronic appendicitis.
He later presented with 12 h of worsening right lower quadrant pain. Examination revealed localized tenderness. Repeat ultrasonography demonstrated a distended, non-compressible appendix measuring 6.4 mm with surrounding fat stranding, increased Doppler flow, a focal wall defect, and moderate ascites, consistent with perforated appendicitis. Complicated Crohn’s disease and infectious appendicitis were considered.
Patient underwent upfront open exploration, which is a common practice in resource limited settings where emergency laparoscopic service is not readily available. The exploration was done via a right lower quadrant transverse incision and it revealed ~400 mL of ascitic fluid, a phlegmonous retrocecal appendix, thickened mesentery (Fig. 1), inflamed terminal ileum, and enlarged mesenteric lymph nodes. The appendiceal base was inflamed, while the cecum appeared grossly normal. An appendectomy was performed, and mesenteric lymph node biopsies were obtained.
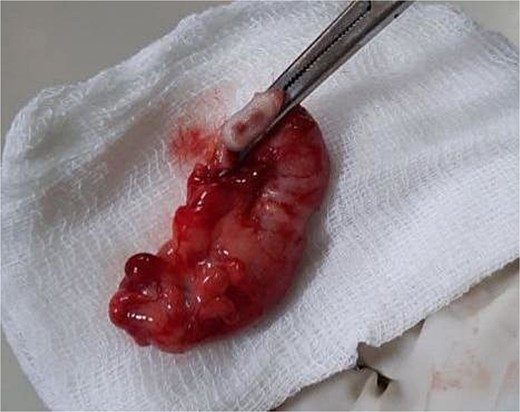
An intraoperative image showing gross morphology of the appendix with thickened wall and mesentery.
Histopathological examination of the appendix demonstrated blanded mucosal epithelium with well-formed granulomas composed of epithelioid histiocytes and multinucleated giant cells, with central caseous necrosis (Fig. 2a–d). These findings were diagnostic of tuberculous appendicitis, and anti-tubercular therapy was initiated.
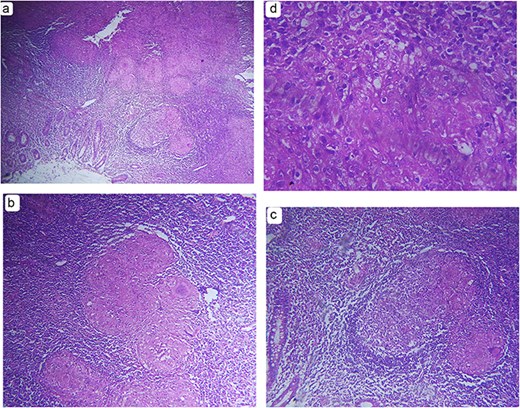
Hematoxylin and eosin–stained sections of the appendix demonstrating features of tuberculous appendicitis. (a) Low-power (×40) photomicrograph showing appendiceal tissue with denuded mucosa and well-formed granulomas composed of epithelioid histiocytes and admixed multinucleated giant cells within a diffuse chronic inflammatory background. (b, c) Intermediate-power (×200) photomicrographs demonstrating granulomas with central caseous necrosis and surrounding epithelioid histiocytes and multinucleated giant cells. (d) High-power (×400) photomicrograph highlighting epithelioid histiocytes arranged in granulomas, consistent with tuberculous inflammation.
The postoperative course was uneventful. The patient completed 6 months of standard anti-tubercular therapy with complete symptom resolution and no recurrence.
Discussion
Tuberculous appendicitis remains an uncommon diagnosis, even in TB-endemic regions. Appendiceal involvement occurs in only 1.5%–3% of patients with abdominal tuberculosis and accounts for ~0.1%–0.3% of all cases of appendicitis [3, 5, 7, 8]. A 2021 literature review identified only 34 reported cases over a 10-year period, indicating its rarity [7]. Most cases occur in young adults from endemic areas, and the absence of concurrent pulmonary involvement or a prior TB history does not exclude appendiceal involvement, as only about one-third of patients demonstrate evidence of prior or active TB elsewhere [7].
The clinical presentation is often indistinguishable from conventional acute appendicitis, contributing to diagnostic delay. While most patients present acutely, a subset report chronic or recurrent abdominal symptoms before acute exacerbation [7, 8]. Our patient’s prolonged course of intermittent diarrhea and tenesmus prior to acute presentation likely reflects the indolent nature of tuberculosis and represents an atypical but recognized manifestation.
Imaging findings are nonspecific and rarely diagnostic. Ultrasonography and computed tomography typically demonstrate features of appendiceal inflammation similar to those seen in pyogenic appendicitis [7, 8]. In this case, serial ultrasonography demonstrated progression from a thickened but compressible appendix to a non-compressible perforated appendix. Associated findings such as mesenteric lymphadenopathy or ascites may suggest tuberculosis but are not definitive [7, 12]. Intraoperative findings are likewise nonspecific, reinforcing the importance of histopathology [8, 10].
The differential diagnosis included Crohn’s disease and other causes of granulomatous appendicitis. Although Crohn’s disease may involve the appendix, granulomas are typically noncaseating and associated with transmural fissures [7, 13]. Infectious etiologies such as Yersinia enterocolitica demonstrate distinct histologic patterns, including suppurative abscess, while sarcoidosis lacks caseation [12, 13]. In this case, the histopathological findings were diagnostic and excluded alternative etiologies.
Once diagnosed, the prognosis of tuberculous appendicitis is generally excellent. Appendectomy provides definitive diagnosis and effective source control, while standard 6-month anti-tubercular therapy eradicates infection. Favorable outcomes have been reported even in cases complicated by perforation when appropriate postoperative therapy is administered [7, 8].
Tuberculous appendicitis is a rare but clinically important entity that should be considered in patients with appendiceal inflammation, particularly in TB-endemic regions or those with atypical or chronic gastrointestinal symptoms. Because clinical and imaging findings are nonspecific, routine histopathological examination of appendectomy specimens remains the cornerstone of diagnosis. Early surgical intervention combined with appropriate anti-tubercular therapy results in excellent outcomes and prevents serious complications.
Conflicts of interest
None declared.
Funding
None declared.
Ethical approval
According to local regulations and the guidelines of Addis Ababa University, ethical approval is not required for case reports provided that patient anonymity is maintained.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

{kind=link}
{kind=link}