





Abstract
Gallbladder volvulus is a rare and frequently underdiagnosed condition, particularly in elderly patients. This case demonstrates a 91-year-old female patient with a clinical presentation of cholecystitis, in which, during the laparoscopy, a gallbladder volvulus was revealed. A detorsion of the gallbladder and cholecystectomy were conducted laparoscopically. Besides minor postoperative complications, the patient was discharged home in the same condition as before surgery. This case highlights that surgical management should be considered in elderly patients with operable cholecystitis to reduce mortality.
Introduction
Gallbladder volvulus is an uncommon clinical entity characterized by twisting of the gallbladder around its axis, which may result in ischemia, necrosis, or perforation if untreated (Figs 1 and 2) [1–3]. It is a rare clinical condition with an estimated incidence of ~1 in 365 000 hospital admissions [1, 3, 4]. The concept of a ‘floating gallbladder,’ predisposing to torsion, was first described by Wendell in 1898 [5]. The condition primarily affects elderly women, with peak prevalence in the seventh and eighth decades of life and a female-to-male ratio of 4:1 in adults [3, 4, 6]. Early diagnosis is challenging, and the condition is often not identified preoperatively [3, 4, 6]. We present a case of clockwise gallbladder volvulus discovered during laparoscopic cholecystectomy in a 91-year-old woman, which was successfully surgically managed.
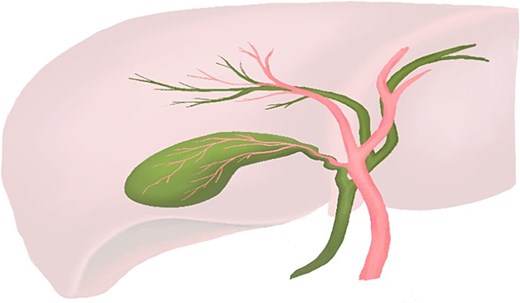
Normal anatomy of the gallbladder, cystic duct, and cystic artery, illustrating the typical fixation of the gallbladder to the liver bed. (Professional medical illustration by Samantha Treyer.)
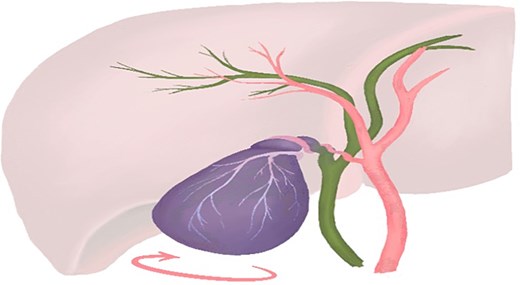
Schematic representation of gallbladder volvulus, showing rotation of the gallbladder around its mesentery and vascular pedicle with resulting vascular compromise. (Professional medical illustration by Samantha Treyer.)
Case report
We report the case of a 91-year-old woman who presented to the emergency room of our hospital with abdominal pain. The patient, weighing 52 kg, has a 12-h history of right upper quadrant abdominal pain accompanied by nausea and vomiting. Her medical history was significant for hypertension and mild cognitive impairment, and no previous abdominal surgeries were registered. Physical examination revealed localized tenderness in the right upper quadrant without signs of peritonitis. Laboratory investigations demonstrated mild leucocytosis (12.54 G/L), with neutrophilia (11.33 G/L) and a C-reactive protein level of 1 mg/L. Liver enzymes were within normal range. Abdominal ultrasound revealed gallbladder hydrops with a longitudinal diameter exceeding 10 cm and gallstones measuring up to 1.6 cm in diameter. The gallbladder wall appeared thickened with partial layering, and the common bile duct measured ~4 mm in the visible segments. There was mild accentuation of the intrahepatic bile ducts. These findings were consistent with acute cholecystitis secondary to cholelithiasis and gallbladder hydrops, necessitating emergency surgical intervention. Given the patient’s good overall fitness, laparoscopic cholecystectomy was appropriately planned. Preoperative care included intravenous ceftriaxone (2 g), analgesia, and fluid resuscitation for optimization before surgery.
Intraoperative evaluation identified a rare condition. The findings included a dark lilac, necrotic, distended, and enlarged gallbladder (Fig. 3a). The gallbladder and cystic duct were attached to the inferior surface of the liver via the mesentery, and the gallbladder was twisted 180° in a clockwise direction. The diagnosis of gallbladder volvulus was established (Fig. 3b). No adhesions, visceral fat, or peritoneal layer were observed near Callot’s triangle, a finding often seen in elderly patients. The torsion was corrected (Fig. 3c), and the haemorrhagic, necrotic gallbladder was removed laparoscopically without complications. The procedure lasted ~1 h, consistent with the standard duration for laparoscopic cholecystectomy at our institution. The patient experienced no anaesthesiologic complications and was transferred postoperatively to the surgical ward.
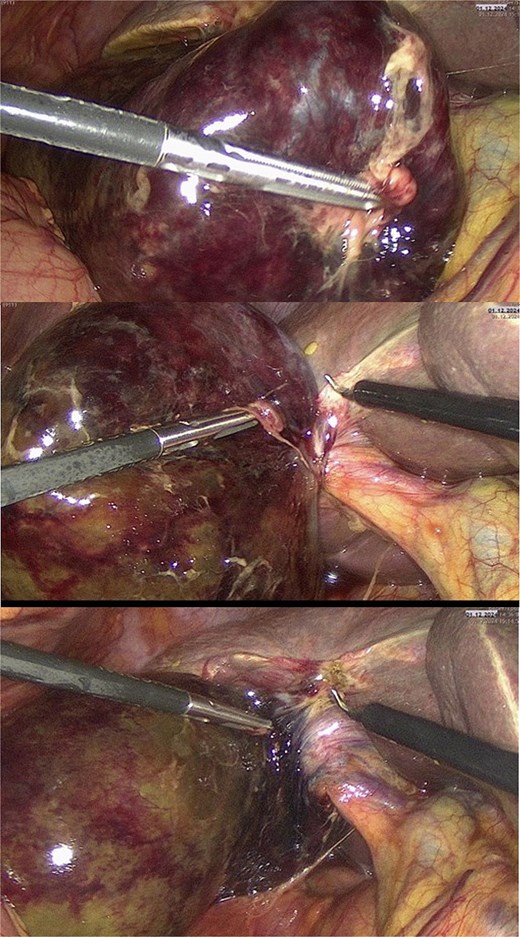
Intraoperative findings in gallbladder volvulus. (a) Distended, gangrenous gallbladder with tense, violaceous wall indicating advanced ischemia. (b) Clockwise volvulus of the gallbladder around the cystic duct and artery, consistent with a floating gallbladder. (c) Appearance after detorsion, with restored anatomical orientation before laparoscopic cholecystectomy.
Postoperative recovery was uneventful. The patient experienced mild postoperative hyperactive delirium, which was managed pharmacologically, resulting in a delayed discharge home. Histological analysis revealed acute gangrenous cholecystitis without evidence of malignancy.
Discussion
This case describes a 91-year-old, thin woman with minimal visceral fat who recovered fully after emergency laparoscopic cholecystectomy, with the diagnosis confirmed intraoperatively due to the limited accuracy of preoperative ultrasound [7, 8]. This case adds to the limited reports of successful minimally invasive management in nonagenarians, supporting the role of surgery in carefully selected elderly patients [6, 9–11].
As summarized in Table 1, our case parallels previous cases in the literature in the diagnosis and management of gallbladder volvulus [4, 6, 9–12]. Reilly et al. reviewed 324 cases and reported preoperative diagnosis in only 26% since 1991, with 6% mortality mainly among elderly patients with comorbidities. Notably, no deaths occurred in those diagnosed preoperatively, highlighting the value of early detection [4]. Recent reports also note successful laparoscopic treatment in octogenarians with risk factors such as low body mass index, prior abdominal surgery, and cancer therapy [3, 6, 9–11].
Comparative table of our case and cases of gallbladder volvulus in the literature.
| Author (year) | Age (years) | Sex | Preoperative diagnosis | Imaging | Treatment |
|---|---|---|---|---|---|
| Croce et al. 2021 | 81 | F | Acute Cholecystitis | CT, US | Laparoscopic Cholecystectomy |
| Reilly et al. 2012 | 77 (Median) | F | Acute Cholecystitis | CT | Laparoscopic Cholecystectomy |
| Ayad Ahmad et al. 2024 | 68 | F | Symptomatic Cholecystolithiasis | US | Laparoscopic Cholecystectomy |
| Bouzas Cardaci et al. 2020 | 88 | F | Acute Cholecystitis DD: Gallbladder Carcinoma | CT, US, MRCP | Diagnostic laparoscopy and Cholecystectomy |
| Wuheb et al. 2025 | 85 | F | Acute Cholecystitis | CT | Laparoscopic Cholecystectomy |
| Azad et al. 2025 | 84 | F | Acute Cholecystitis | CT | Laparoscopic Cholecystectomy |
| Present case | 91 | F | Acute Cholecystitis | US | Laparoscopic Cholecystectomy |
Preoperative imaging for gallbladder volvulus is often nonspecific and can resemble acute cholecystitis on ultrasound [7]. Ultrasound may show distension and wall thickening but rarely demonstrates clear signs of volvulus [7, 8]. Computed tomography (CT) can identify a displaced gallbladder, ‘whirl sign,’ and ischemia. Magnetic resonance imaging or magnetic resonance cholangiopancreatography (MRCP) with diffusion-weighted imaging can confirm cystic duct torsion and ischemia, thereby enabling an accurate preoperative diagnosis [8, 13–15].
In elderly women with right upper quadrant pain and distension, gallbladder volvulus should be suspected, and advanced imaging should be considered [7, 14]. In this case, only an ultrasound was performed due to the urgency of surgery. Awareness of CT and MRCP findings may facilitate earlier diagnosis [8, 13, 14]. Emergency laparoscopic cholecystectomy was appropriate given the patient’s fitness, as early surgery improves outcomes in selected elderly patients [3, 4, 6, 9–11]. Prompt management can prevent gangrene and perforation. Laparoscopy reduces pain, hospital stay, and recovery time, offering advantages in older adults [3, 6, 10, 11].
Postoperative delirium highlighted the need for geriatric assessment and prevention strategies. Early mobilization led to full recovery, demonstrating that surgery is safe when functional reserves are adequate and that conservative care is risky [4, 10, 11]. Preoperative diagnosis via advanced imaging, though rare, improves outcomes and with mortality near 6% in delayed or comorbid cases, this recovery at 91 supports surgical management in the very elderly [3, 4, 6].
This case underscores the need to recognize gallbladder volvulus in elderly women with acute cholecystitis and to include it in the differential diagnosis, reaffirming the value of laparoscopic treatment in acute cases.
Conclusion
Gallbladder volvulus should be suspected in elderly patients with acute cholecystitis, with early laparoscopic cholecystectomy as the preferred treatment for those with good functional status.
Conflicts of interest
None declared.
Funding
None declared.
Declaration of patient consent
The patient has given consent for his images and other clinical information to be reported. A signed consent form is available.
Guarantors
Stefan Breitenstein, Patryk Kambakamba.

{kind=link}
{kind=link}
{kind=link}