





Abstract
Acute appendicitis is a common surgical emergency, and antibiotic therapy is a safe and effective alternative to surgery for computed tomography (CT)-confirmed uncomplicated cases. Rarely, an underlying appendiceal tumor may present as acute or recurrent appendicitis. We report the case of a man in his early 60s with CT-confirmed uncomplicated appendicitis who initially recovered with antibiotics but re-presented 6 weeks later with recurrent symptoms. Laparoscopic appendectomy revealed a goblet cell adenocarcinoma (GCA, pT4a) of the appendix with lymphatic and perineural invasion. Staging imaging showed no synchronous colorectal lesions or metastases. Completion right hemicolectomy demonstrated no residual tumor or lymph node involvement (0/26; final stage pT4N0M0). Adjuvant chemotherapy was not administered, and at 1-year follow-up the patient remains disease-free. This case highlights that although appendiceal malignancy is rare in uncomplicated appendicitis, recurrence should prompt definitive surgical management and careful pathological evaluation, particularly in adults.
Introduction
Acute appendicitis is a common surgical emergency, and antibiotics have emerged as a safe and effective alternative to appendectomy for computed tomography (CT)-confirmed uncomplicated cases in adults [1]. In the Appendicitis Acuta (APPAC) randomized clinical trial enrolling patients aged 18–60 years, long-term follow-up demonstrated durable outcomes after initial antibiotic therapy, with a histologically confirmed recurrence rate of 37.8% and a cumulative appendectomy rate of 44.3% at 10 years [2]. These data support antibiotics as an evidence-based option, provided patients are counseled regarding recurrence risk [2].
A persistent concern with increasing non-operative management is the possibility of an occult appendiceal neoplasm remaining undiagnosed in the absence of surgical pathology. This concern is especially relevant in older patients, who have higher baseline risk of appendiceal tumors [3]. Available evidence suggests that appendiceal tumor risk is closely associated with disease severity, underscoring the importance of distinguishing uncomplicated from complicated appendicitis [2, 4]. In the 10-year follow-up of the APPAC trial, the prevalence of appendiceal tumors among patients initially treated with antibiotics was 0.9%, with an overall tumor prevalence of 1.2% among patients with uncomplicated acute appendicitis [2].
Goblet cell adenocarcinoma (GCA) is a rare appendiceal malignancy characterized by mixed glandular and neuroendocrine differentiation [5]. Previously termed “goblet cell carcinoid,” it is now classified as an adenocarcinoma because of its aggressive clinical behavior [5]. GCA accounts for ~5%–15% of primary appendiceal neoplasms, depending on the series and classification used [6–8]. Clinically, it frequently presents as acute appendicitis and is often diagnosed only after appendectomy and histopathological examination [6]. Given its propensity for transmural invasion and regional or peritoneal spread, oncologic resection with right hemicolectomy is commonly recommended when GCA is identified, particularly in the presence of adverse pathological features [6–8].
We report a case in which recurrent uncomplicated appendicitis after initial antibiotic treatment led to the diagnosis of an appendiceal goblet cell adenocarcinoma.
Case report
A man in his early 60s presented with a 2-week history of right lower quadrant abdominal pain, accompanied by low-grade fever. Laboratory tests showed a normal white blood cell count (8.2 × 109/L) and elevated CRP. Contrast-enhanced abdominal computed tomography (CT) confirmed uncomplicated acute appendicitis with focal thickening at the appendiceal tip (maximum diameter ~11 mm) and periappendiceal fat stranding (Fig. 1). There was no abscess, perforation, appendicolith, or mass, and the cecum appeared unremarkable.
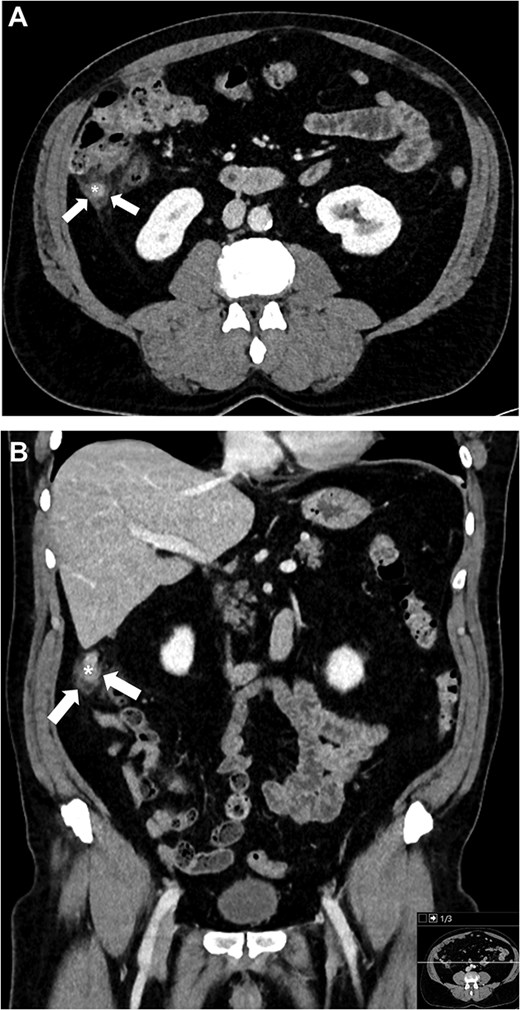
Contrast-enhanced CT images of the abdomen at the initial presentation, demonstrating an inflamed appendix with focal thickening at the appendiceal tip (*) and periappendiceal fat stranding (arrows) on axial (A) and coronal (B) planes.
After discussion of management options, including operative and non-operative strategies supported by randomized trials, the patient preferred to avoid surgery. He was treated as an outpatient with oral moxifloxacin 400 mg once daily for seven days, following a regimen evaluated in trials for uncomplicated appendicitis [1, 9, 10]. His symptoms resolved rapidly, and he recovered uneventfully without surgery.
Approximately 6 weeks later, the patient returned with acute right lower quadrant pain and localized tenderness similar to his prior presentation. He was febrile on presentation and hemodynamically stable. Laboratory studies showed leukocytosis (15.1 × 109/L) and an elevated C-reactive protein level of 48 mg/L. Repeat contrast-enhanced CT confirmed recurrent uncomplicated appendicitis with a dilated, inflamed appendix (especially at the tip) and surrounding inflammatory changes, again without any appendicolith, abscess, perforation, or radiologically visible tumor (Fig. 2).
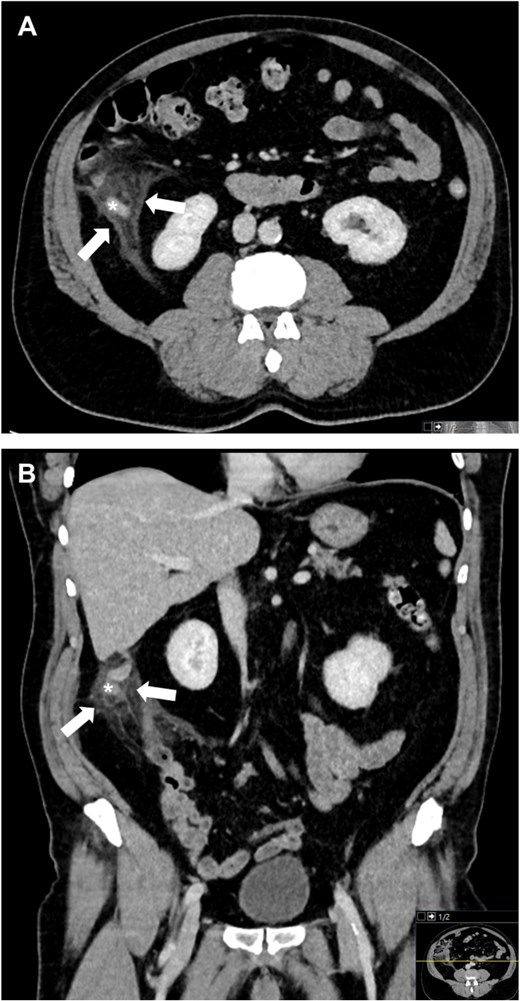
Contrast-enhanced CT images of the abdomen at the recurrence, again showing an inflamed appendix with pronounced thickening at the tip (*) and periappendiceal fat stranding (arrows) in axial (A) and coronal (B) planes.
Given the recurrence despite appropriate antibiotic therapy, a laparoscopic appendectomy was performed. Intraoperatively, the appendix was inflamed at the tip without perforation, abscess, or generalized peritonitis, and no macroscopic tumor implants were observed. The appendectomy was completed without complication; no postoperative antibiotics were administered, and the patient was discharged on postoperative day one.
Histopathological examination of the appendectomy specimen unexpectedly revealed a goblet cell adenocarcinoma arising in the distal appendix. The tumor had invaded through the muscularis propria into the subserosa (pT4a) and showed perineural and lymphatic invasion, with no definite venous invasion. The proximal resection margin was free of tumor, and mismatch repair protein expression was intact, indicating microsatellite stability.
After multidisciplinary tumor board review, a completion right hemicolectomy was recommended for oncologic clearance and lymph node staging. The patient underwent a laparoscopic right hemicolectomy ~2 months later. Histopathological analysis of the colectomy specimen demonstrated no residual tumor and no lymph node metastases among 26 retrieved nodes (0/26), yielding a final pathological stage of pT4N0M0 (stage IIB). Adjuvant chemotherapy was not administered. At 1-year follow-up, the patient remains asymptomatic and disease-free under structured surveillance.
Discussion
This case illustrates a rare scenario of a goblet cell adenocarcinoma discovered after recurrent CT-confirmed uncomplicated appendicitis initially managed with antibiotics. However, in the APPAC trial 10-year follow-up, appendiceal tumors were identified in only 0.9% of patients after initial antibiotic management, similar to the 1.2% prevalence among all uncomplicated cases [2]. These findings confirm that antibiotic therapy does not increase cancer risk compared to immediate appendectomy. Instead, tumor risk correlates with disease severity and is higher in complicated appendicitis (e.g. perforation or abscess [2, 4, 11]).
This case is an exception to current evidence, as the patient met radiological criteria for uncomplicated appendicitis at both presentations without any complicating features on CT, and his initial antibiotic management followed protocol [10]. An early recurrence is not surprising after non-operative management, since most recurrences occur within the first year after antibiotic treatment [1, 2, 10]. Thus, recurrence should prompt surgery.
Goblet cell adenocarcinoma often presents as acute appendicitis and is usually diagnosed after an appendectomy [6–8]. On imaging, it typically lacks a discrete mass due to diffuse infiltration, which explains the absence of a visible tumor on CT. Given its propensity for transmural invasion and regional spread, a completion right hemicolectomy is generally recommended even if the appendectomy margins are negative [5–8]. In our patient, the hemicolectomy confirmed no residual tumor or nodal metastases. No adjuvant chemotherapy was given, as evidence is limited [5, 7, 8]. Close surveillance is warranted.
In conclusion, antibiotic therapy is a safe, evidence-based treatment for CT-confirmed uncomplicated appendicitis, but rare malignancies such as GCA may present as recurrent appendicitis. These observations do not undermine the APPAC evidence base, but highlight the need for definitive surgery and thorough evaluation when appendicitis recurs.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}