





Abstract
Chronic distal biceps tendon ruptures present significant reconstructive challenges due to tendon retraction, scarring, and muscle atrophy. Allograft-based reconstruction is a viable option for delayed presentations, particularly in high-demand individuals. We report the case of a 33-year-old male bodybuilder who presented 2 years after sustaining a distal biceps rupture. Examination revealed a reverse Popeye deformity, marked weakness, and magnetic resonance imaging evidence of complete tendon rupture with substantial retraction and muscle atrophy. Surgical reconstruction was performed using an Achilles tendon allograft secured proximally with a Pulvertaft weave and distally with a cortical button fixation device (EndoButton™, Smith & Nephew, Memphis, TN, USA) following preparation and tensioning of the graft. Rehabilitation progressed from immobilization to full return to lifting by 6 months. Preoperatively, the patient reported a QuickDASH score of 54.54, indicating substantial upper-extremity disability. At 7 months postoperatively, the patient demonstrated full, pain-free elbow motion; symmetric flexion and supination strength; and restored biceps contour. The QuickDASH improved to 25.0, and the Oxford Elbow Score reached 48/48, reflecting marked functional recovery. Radiographs confirmed absence of heterotopic ossification or fixation-related complications. This case highlights the feasibility and favorable short-term functional outcomes of Achilles allograft reconstruction for chronic distal biceps ruptures, even in patients presenting more than a year after injury. These findings support Achilles allograft reconstruction as a viable option in selected high-demand individuals with neglected injuries.
Introduction
Distal biceps tendon ruptures are considered chronic when treatment is delayed beyond 3–6 weeks after injury [1, 2]. Although relatively uncommon, with a reported prevalence of 1.2–2.55 per 100 000 person-years, chronic cases account for ~ 19% of all distal biceps repairs and predominantly affect middle-aged men engaged in physically demanding activities [1–3]. Progressive tendon retraction, scarring, and compromised tissue quality make delayed presentations particularly challenging to manage.
The incidence of distal biceps ruptures has increased substantially over recent decades, rising from 1 per 100 000 in 2001 to 6 per 100 000 in 2015, likely reflecting increased participation in resistance training and other high-demand upper-extremity activities [3]. Established risk factors include smoking, obesity, corticosteroid use, and overexertion, with smokers demonstrating a 7.5-fold increased risk compared with non-smokers [2, 4].
Acute ruptures typically present with sudden pain, an audible pop, swelling, and weakness in elbow flexion or forearm supination [5]. In contrast, chronic ruptures more commonly result in persistent strength deficits, activity-related fatigue, and a characteristic inverse Popeye deformity secondary to tendon retraction [6].
Surgical reconstruction remains the treatment of choice for chronic distal biceps ruptures and frequently requires graft augmentation to address severe retraction and poor tendon quality [7]. Favorable outcomes have been reported following reconstruction, with recovery of ~ 90% of contralateral supination strength and 62% of flexion strength, despite some expected residual deficits [2]. Comparative studies suggest that delayed repairs performed after 21 days can achieve functional outcomes comparable to acute repairs, with reported recovery of 89% flexion and 77% supination strength relative to the uninjured side [8]. High patient satisfaction following graft-based reconstruction has also been consistently reported [9]. While acute repairs may be associated with higher rates of transient neurological complications, heterotopic ossification appears more frequently reported in acute rather than chronic cases [1, 8].
This case highlights the unique challenges of reconstructing a chronic distal biceps tendon rupture in a bodybuilder > 2 years after injury. Severe tendon retraction, mild-to-moderate muscle atrophy, and a pronounced inverse Popeye deformity necessitated reconstruction using an Achilles tendon allograft secured with cortical fixation. Although chronic distal biceps ruptures are variably defined, most reconstructions reported in the literature are performed within 6–12 weeks of injury, with average delays ranging from 60 to 75 days [10]. Reporting this case contributes valuable insight into managing extreme chronicity in high-demand patients.
Case presentation
A 33-year-old male bodybuilder presented with progressive left arm weakness, pain, and a visible biceps deformity. He sustained an injury during powerlifting 2 years earlier and did not seek medical attention. He denied smoking and anabolic steroid use. Examination showed a pronounced inverse Popeye deformity with full elbow range of motion. The distal biceps tendon was palpable but non-tensioned, and the hook (Roland) test was positive (Fig. 1A and B). Magnetic resonance imaging (MRI) confirmed a complete distal biceps tendon rupture with marked proximal retraction and moderate muscle atrophy (Fig. 2A and B). Preoperatively, the patient reported a QuickDASH score of 54.54, indicating significant upper-extremity functional impairment.
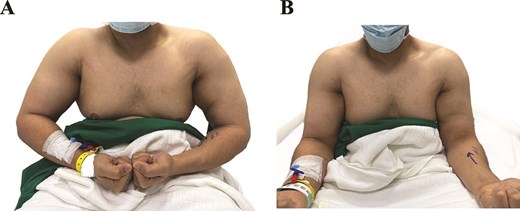
(A) Preoperative image with the elbows flexed to 90°, demonstrating asymmetry and distal flattening of the left biceps contour, consistent with a reverse Popeye deformity of chronic distal biceps rupture. (B) Preoperative image in a neutral arm position showing loss of distal biceps tension on the left side.
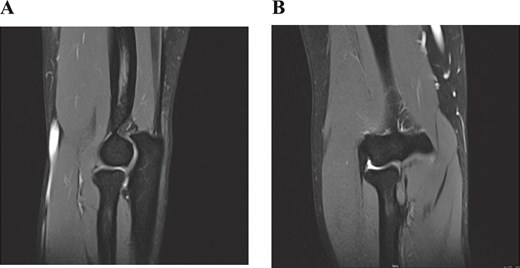
(A) Sagittal T2-weighted MRI demonstrating marked proximal retraction of the ruptured distal biceps tendon. (Label: ‘Retracted tendon stump.’). (B) Coronal T2-weighted MRI showing absence of the distal tendon at the radial tuberosity, consistent with a full-thickness rupture. (Label: ‘Absent tendon at insertion.’).
Reconstruction was performed under general anesthesia with the patient supine. A Lazy-S incision was made over the antecubital fossa. The tendon stump was identified ~ 15 cm proximally and appeared fibrotic and degenerated; it was debrided. The lateral antebrachial cutaneous nerve, brachial artery, and posterior interosseous nerve were identified and protected.
A tendon-only Achilles allograft (without calcaneal bone block) was selected to restore tendon length. The graft was prepared on the back table and trimmed to allow adequate proximal overlap for Pulvertaft weaving while maintaining sufficient distal length for anatomic fixation at the radial tuberosity. The graft ends were whip-stitched with nonabsorbable sutures to facilitate handling and fixation. The graft was secured proximally to the muscle–tendon junction using a Pulvertaft weave (Fig. 3A). Corner sutures were placed at each graft passage through the native tissue, and the graft was reinforced by suturing it to itself to enhance construct strength.

(A) Intraoperative image showing the Achilles tendon allograft weaved into the retracted biceps muscle belly using a Pulvertaft technique through a single anterior approach. The prepared graft length was approximately 15 cm. (B). Distal fixation of the allograft into the radial tuberosity using a transosseous EndoButton following tensioning with the elbow positioned at 90° flexion and 50° supination.
Tension was set with the elbow in slight flexion and supination, and the construct was reinforced with additional sutures. Anchoring the graft in chronic reconstructions presents technical challenges due to muscle atrophy, graft–host mismatch, and the risk of overtensioning or fixation failure. To mitigate these risks, graft tension was adjusted incrementally and stability was confirmed through a full arc of elbow motion prior to closure.
Distally, a 4.5-mm tunnel was drilled at the radial tuberosity, and fixation was achieved with a transosseous cortical button fixation device (EndoButton™, Smith & Nephew, Memphis, TN, USA) with the elbow held at 90° flexion and 50° supination (Fig. 3B). Stability and tension were confirmed through elbow motion, the wound was closed in layers, and the limb was immobilized in a posterior splint at 90° flexion and 50° supination.
The patient was immobilized for 6 weeks, then began passive motion at week six and active motion at week eight. Strengthening started at 12 weeks, with return to unrestricted weightlifting at 6 months.
At 7 months, he had a stable, well-tensioned reconstruction and a full, pain-free range of motion (Fig. 4A and B), with symmetric strength versus the contralateral side. The QuickDASH improved from 54.54 preoperatively to 25.0 at final follow-up, and the Oxford Elbow Score reached 48/48, demonstrating substantial functional recovery. Wound healing was complete; sensory and motor examinations were normal, including lateral antebrachial cutaneous and posterior interosseous nerve function. Postoperative radiographs obtained in October 2025 demonstrated stable cortical button fixation without hardware migration, heterotopic ossification, radioulnar synostosis, or other fixation-related complications (Fig. 5).
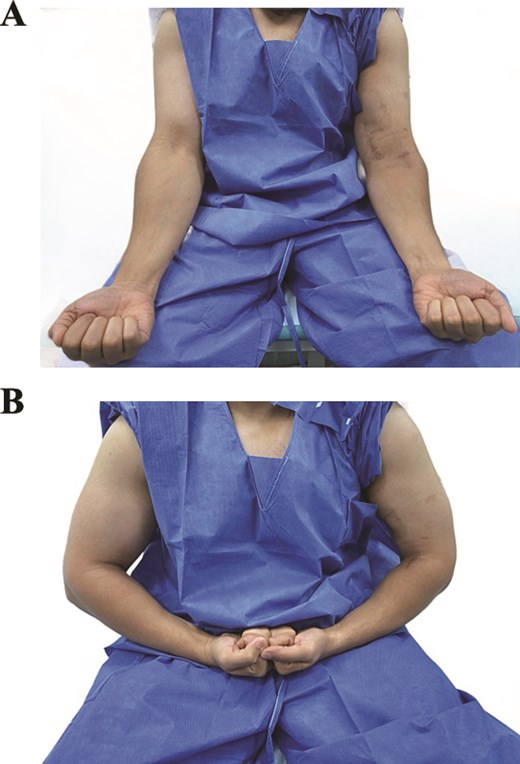
(A) Postoperative clinical image demonstrating restoration of normal biceps contour on the operated (left) side. (B) Postoperative image during active elbow flexion showing symmetric biceps bulk compared to the contralateral limb, indicating excellent cosmetic and functional recovery.
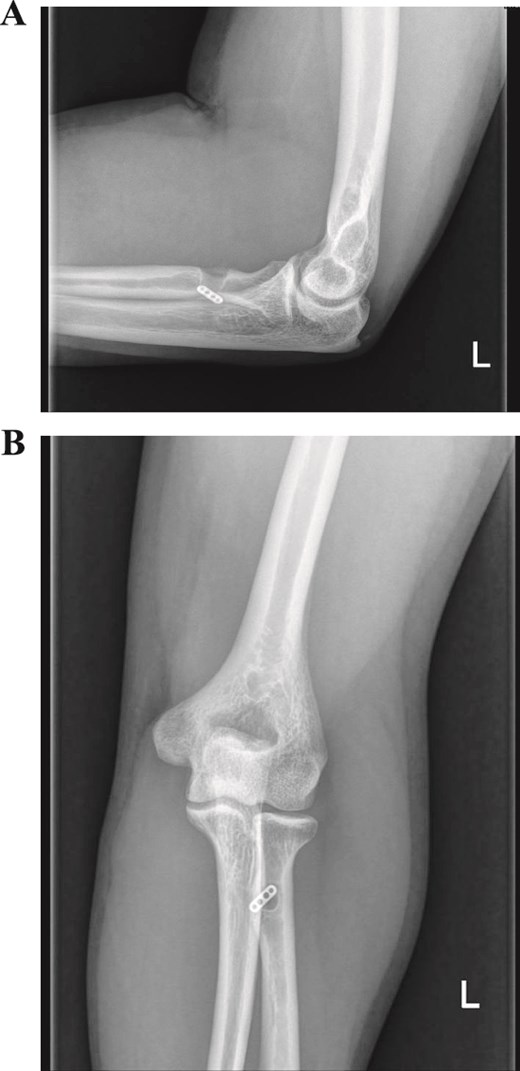
Postoperative anteroposterior (A) and lateral (B) radiographs of the left elbow obtained 7 months after Achilles tendon allograft reconstruction (October 2025), demonstrating stable cortical button fixation at the radial tuberosity without evidence of hardware migration, heterotopic ossification, radioulnar synostosis, or other fixation-related complications.
Discussion
Chronic distal biceps tendon ruptures are uncommon and present unique challenges due to progressive tendon retraction, tissue degeneration, and muscle atrophy when treatment is delayed beyond 3 weeks. Our patient exhibited classic features of chronic rupture, including a pronounced inverse Popeye deformity, weakness in elbow flexion and forearm supination, and MRI evidence of tendon retraction and muscle atrophy. In such cases, reconstruction using an allograft combined with cortical button fixation represents a reliable option to restore tendon length and function.
Cortical button fixation has been widely adopted in both acute and chronic distal biceps repairs and is associated with high patient satisfaction and favorable functional outcomes [11]. In chronic ruptures, this technique offers the advantage of strong fixation capable of withstanding early rehabilitation despite compromised tendon quality and pre-existing stiffness [11]. Panagopoulos et al. reported satisfactory restoration of elbow flexion–extension in 89.5% of patients and pronation–supination in 82% following chronic reconstructions using cortical button fixation, supporting its effectiveness in delayed presentations [11].
Despite these benefits, complication rates are generally higher in chronic repairs due to increased technical complexity and poor tissue quality. Hamer et al. reported major and minor complication rates of 7.8% and 33.3%, respectively, after acute repair, with even higher rates observed in chronic cases. Overall complication rates for distal biceps repair approach 25%, with nerve-related complications being the most common. Lateral antebrachial cutaneous nerve irritation occurs in ~ 9.2% of cases, while posterior interosseous nerve palsy has been reported in 1.6%. Other complications include rerupture (1.4%), heterotopic ossification (2.9%), and rare vascular injuries (<0.1%). Technique-related complications, such as proximal radioulnar synostosis, vary by surgical approach, with higher rates reported in more extensile single-incision techniques [1, 6, 8, 12–16]. One study demonstrated a complication rate of 46% in repairs performed after 4 weeks, compared with 30% in acute cases [1–3, 6, 8, 9, 11–19].
Although delayed reconstructions performed > 1 year after injury are rare, successful outcomes have been reported using a variety of graft options, including Achilles tendon, semitendinosus, lacertus fibrosus, and acellular dermal matrix grafts [2, 3, 5, 10, 11, 18, 19]. The Achilles tendon allograft offers several advantages in chronic reconstructions, including sufficient length, robust tensile strength, and ease of handling, which facilitate restoration of tendon length in the setting of marked proximal retraction. In contrast, semitendinosus autografts provide a biologic alternative but may be limited by donor-site morbidity and insufficient graft length in markedly delayed cases. Lacertus fibrosus augmentation may be suitable in select patients with preserved native tissue but is often inadequate in advanced degeneration. Acellular dermal matrix grafts avoid donor-site morbidity; however, concerns remain regarding long-term structural integrity in high-demand individuals.
Case series consistently demonstrate that even markedly delayed reconstructions can provide meaningful pain relief, improved function, and high patient satisfaction, with most complications being minor and transient [7, 20]. Common reconstruction techniques include Pulvertaft weave augmentation, transosseous tunnels, and cortical button fixation devices such as the EndoButton™ (Smith & Nephew, Memphis, TN, USA) [2, 3, 5, 7, 10, 11, 18–20]. Functional outcomes assessed using validated measures—including the QuickDASH, Oxford Elbow Score, and Mayo Elbow Performance Score—are generally good to excellent, with most patients able to return to pre-injury activity levels, including high-demand sports [2, 3, 5, 10, 11, 18–20].
In the present case, substantial improvement in QuickDASH score from 54.54 preoperatively to 25.0 at 7 months, together with restoration of strength and motion, supports the effectiveness of Achilles allograft reconstruction in the short term. However, longer follow-up is necessary to determine durability of these outcomes.
Conclusion
This case demonstrates the successful reconstruction of a severely retracted chronic distal biceps tendon rupture in a high-demand patient using an Achilles tendon allograft. Despite a 2-year delay from injury to treatment, the patient achieved excellent cosmetic restoration, full range of motion, and outstanding functional outcomes. These results reinforce the feasibility, durability, and clinical effectiveness of allograft reconstruction for neglected distal biceps ruptures, especially in individuals with high functional expectations. This case adds to the growing evidence supporting reconstruction as a reliable option even in markedly delayed presentations.
Conflicts of interest
None declared.
Funding
None declared.
Ethical approval
This study was reviewed and approved by the institutional review board (IRB Approval No: E-2655). All procedures were conducted in accordance with applicable ethical standards and the principles of the Declaration of Helsinki. Where applicable, informed consent was obtained from participants or their legal guardians.
References
Elbowadmin. Chronic distal biceps tendon rupture-ElbowDoc. London, UK: ElbowDoc; 2022 Nov 2. [Internet]. Available from: https://www.elbowdoc.co.uk/chronic-distal-bicepstendon-rupture/

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}