





Abstract
Gossypiboma is a diagnostic challenge, particularly in long-standing cases where characteristic imaging features may be lost. We report the case of a 78-year-old woman with a sponge retained from an abdominal hysterectomy performed 38 years earlier. The pelvic mass was incidentally detected on computed tomography (CT) and misdiagnosed as a solid ovarian tumor on magnetic resonance imaging, prompting a laparotomy. Intraoperatively, the mass was revealed to be a retained sponge; however, complete resection was impossible due to severe adhesions and massive bleeding. During follow-up without reoperation, the patient developed abdominal pain 16 months later, and CT showed a small bowel fistula and an intra-abdominal abscess. Due to the high surgical risk and the fact that resection of the mass would be extremely difficult, a diverting loop ileostomy was created to control the inflammation. This case highlights the difficulty of preoperative diagnosis and discusses optimal management strategies for long-standing, asymptomatic gossypiboma.
Introduction
Gossypiboma is a surgical sponge retained after a surgical procedure, with a reported frequency of ~1 in 1000–1500 surgeries [1]. Although any surgical field carries risk, abdominal surgeries are most frequently implicated [2]. Gossypibomas act as foreign bodies, often causing fever and pain. When radiopaque markers are present, detection is relatively straightforward; however, with prolonged retention, characteristic imaging features may be lost, making diagnosis difficult [3]. In the present case, an ovarian tumor was suspected preoperatively, and a pelvic gossypiboma was identified only during laparotomy, where complete resection was not feasible. Sixteen months later, an enteric fistula developed, necessitating a diverting loop ileostomy to control infection. Here, we report the clinical course and management of this long-standing gossypiboma.
Case report
A 78-year-old woman (gravida 3, para 2), with hypertension and hyperlipidemia, was receiving medical treatment. She had undergone an appendectomy at 13 years, surgery for an ectopic pregnancy at 23 years, and a total hysterectomy at 40 years, all via laparotomy. Details of the hysterectomy were unavailable owing to the long interval. Nine years earlier, abdominal computed tomography (CT) performed for a pancreatic cyst incidentally revealed a right pelvic mass. Contrast-enhanced magnetic resonance imaging (MRI) showed a 4.5 cm lesion, with mixed signal intensity on T2-weighted imaging and mild peripheral enhancement, leading to a preoperative diagnosis of a solid ovarian tumor. As she was asymptomatic, conservative follow-up was chosen. Eight years later, MRI showed enlargement of the lesion to 6 cm (Fig. 1), with internal fluid accumulation. An ovarian fibroma, Brenner tumor, or mucinous cyst was suspected. Laparotomy was performed for tumor resection. At the surgery, the retroperitoneal pelvic mass was identified, firmly adherent to the intestine. Central necrotic and fibrotic tissue was observed; however, massive bleeding occurred, and only a biopsy was performed. The operation time was 3 h 33 min, with a blood loss of 1510 g, requiring transfusion of two units of red blood cells and fresh frozen plasma. She was discharged on post-operative Day 9. Histological examination revealed fibrous tissue with cross-sections of gauze fibers and multinucleated giant cell granulomas, confirming gossypiboma (Figs 2 and 3). Given the retroperitoneal location, the lesion was presumed to have originated from gauze retained during a hysterectomy performed 38 years earlier.
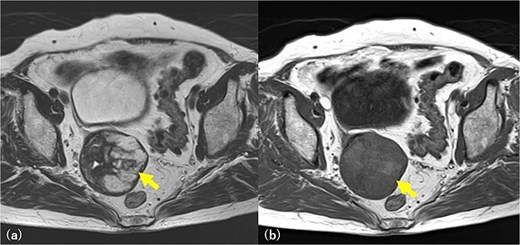
Pelvic MRI imaging. A 6 cm diameter solid mass is found in the right pelvic wall and is suspected to be an ovarian fibroma and Brenner tumor. T2-weighted image, a multilocular high signal, and fluid accumulation are revealed (arrow) (a). The same area is slightly detected as a high signal in the T1-weighted image (arrow) (b), and a mucinous tumor is also suspected.

Surgical specimen. The presence of gauze-like fibrous tissue is noted accompanying the granuloma (arrow).
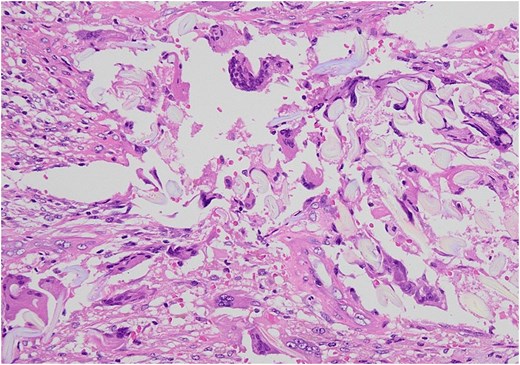
Microscopic examination showed by H&E × 200 staining. Foreign body granuloma containing a piece of gauze and giant cells.
Transvaginal ultrasonography at 1 and 6 months showed no change. Sixteen months postoperatively, she presented with abdominal pain. CT revealed a fistula with the small intestine and also demonstrated abscess formation between the residual mass and small intestine, with an abscess between the mass and bladder (Fig. 4), accompanied by elevated inflammatory markers. As repeat excision was considered high risk, surgical management focused on controlling inflammation by eliminating intestinal communication. A diverting double-barrel loop ileostomy was therefore planned laparoscopically. A trocar was first placed at the umbilicus for the laparoscope, and additional trocars were placed in the right lateral and lower abdomens. Severe adhesions were encountered, necessitating the placement of additional trocars in the left lateral and lower abdomens. The small intestine was looped and clustered on the right pelvic floor; however, the gossypiboma could not be identified. The terminal ileum in the caecum was identified, and the fistula site was determined to be ~17 cm proximal to the ileocecal junction. A double-barrel stoma was created 10 cm proximal to the fistula site in the right lower abdomen (Fig. 5). After confirming her ability to manage the stoma and tolerate oral intake, she was discharged on post-operative Day 24. To date, no recurrence of the pelvic inflammation has been reported. The overall clinical course of the present case is summarized in the timeline (Fig. 6).
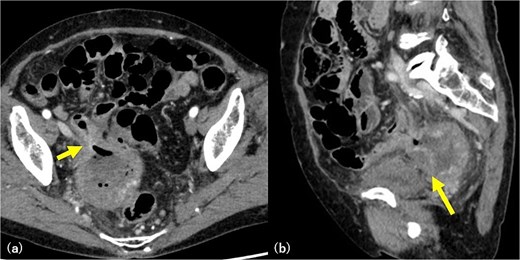
Abdominal CT imaging. Axial CT image showing intralesional air within the gossypiboma, indicating communication with the small intestine (arrow) (a). Sagittal CT image demonstrating fluid collection between the mass and the bladder, consistent with abscess formation secondary to rupture (arrow) (b).
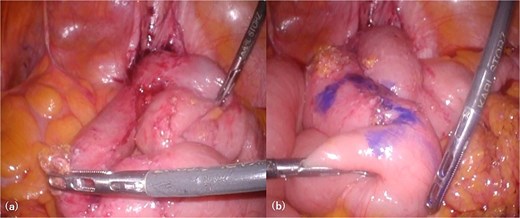
Intra-abdominal findings. The right side of the image corresponds to the patient’s right side. Looped small bowel segments are clustered along the right pelvic peritoneum, and despite adhesiolysis, the entirety of the gossypiboma could not be identified (a). The site for stoma creation is marked ~10 cm proximal to the afferent limb of the loop (b).
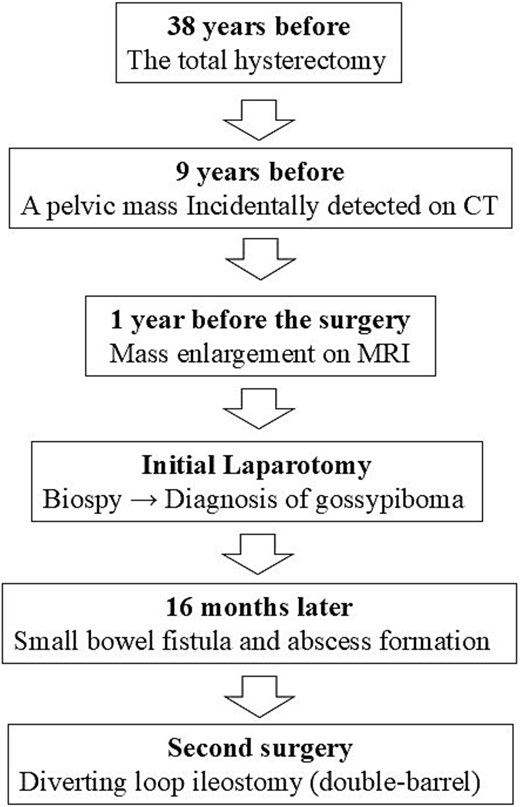
Clinical timeline of the present case.
Discussion
Gossypiboma is a retained surgical sponge, and ~53% of reported cases occur after gynecological surgery. However, the true incidence remains unknown because such events often involve medicolegal implications and may be misdiagnosed [4]. Reported risk factors include emergency surgery, intraoperative changes in the procedure, uncontrolled bleeding, and obesity [5]. Clinical manifestations vary from pain and fever to fistula formation, abscess formation, or bowel obstruction caused by adhesions or intraluminal migration of the sponge. Nevertheless, ~6% of cases remain asymptomatic [6]. Once diagnosed, surgical resection is generally recommended [7]. Importantly, the optimal surgical strategy should be individualized according to the degree of adhesion, inflammatory involvement, and patient condition. In long-standing cases, dense adhesions and severe inflammatory changes may make complete excision hazardous, with a substantial risk of bleeding or bowel injury. In such situations, staged management, including temporary fecal diversion, may represent a safer alternative to aggressive resection. In the present case, extensive adhesions precluded safe complete excision, and a diverting loop ileostomy was constructed to control contamination and allow infection management.
Histopathologically, gossypibomas are known to elicit two types of reactions: exudative reaction, leading to abscess or fistula formation, and aseptic reaction, resulting in granuloma formation. In the present case, an aseptic fibrinous reaction likely developed before laparotomy, whereas an exudative reaction occurred later, leading to fistula formation and inflammatory exacerbation [8].
Although the details of the hysterectomy performed 38 years earlier were unavailable, preoperative imaging did not suggest gossypiboma. A history of prior surgery should prompt inclusion of gossypiboma in the differential diagnosis. Due to severe adhesions and bleeding, complete excision during laparotomy could not be achieved, which ultimately resulted in abscess formation and small bowel fistula 1 year later. Previously asymptomatic gossypibomas may become clinically significant after surgical manipulation, eventually necessitating diverting loop ileostomy creation and imposing a substantial burden on the patient. Early recognition may influence surgical planning and referral decisions, potentially allowing complete excision under safer conditions.
In conclusion, gossypiboma should always be considered in patients with a history of surgery. In this case, preoperative diagnosis was not achieved, and subsequent surgical manipulation precipitated fistula formation. As surgical removal remains the only definitive treatment, preoperative suspicion and complete excision should be pursued whenever feasible, even when technically challenging. Ongoing preventive measures remain essential to avoid retained surgical materials in future practice.
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}