





Abstract
Small bowel obstruction (SBO) following blunt abdominal trauma (BAT) is an uncommon but important delayed complication, usually resulting from ischemic or fibrotic changes secondary to mesenteric injury. A 52-year-old male presented 2 months after BAT with a 5-day history of progressive bowel obstruction. Computed tomography imaging showed a 10-cm distal ileal stenosis with mural thickening and mesenteric hyperemia. Exploratory laparotomy revealed a 4-cm ileal thickening and mesenteric laceration. A 20-cm ileal resection with latero-lateral isoperistaltic anastomosis was performed. Histology confirmed ischemic injury secondary to local trauma. This case illustrates a rare presentation of delayed SBO due to post-traumatic mesenteric ischemia. Clinicians should maintain a high index of suspicion in patients with prior BAT and evolving gastrointestinal symptoms to ensure timely diagnosis and management.
Introduction
The most frequent causes of small bowel obstruction (SBO) include postoperative adhesions, hernias, neoplasms, and inflammatory strictures [1]. Although blunt abdominal trauma (BAT) predominantly causes solid organ injuries, bowel injuries represent a less frequent but clinically significant subset [2, 3] Post-traumatic SBO, although rare, may occur due to the formation of intramural or mesenteric hematomas, ischemic injury, and fibrotic strictures developing days to weeks after the initial trauma. We present a case of delayed SBO obstruction following BAT.
Case presentation
A 52-year-old male with a personal history of type II diabetes, chronic liver disease, due to alcohol intake, and gallstones was admitted to our Emergency Department with a 5-day history of progressive SBO. Abdominal tenderness was present, but no signs of guarding were found. Bowel sounds were absent and the percussion note was tympanitic throughout the abdomen. Laboratory investigations revealed only leukocytosis (WBC 13.8 × 103/μl), elevated C-reactive protein of 6.46 mg/dl (normal < 0.5 mg/dl), and an International Normalized Ratio (INR) of 1.9. A naso-gastric tube was inserted, and 500 ml of fecaloid content was drained.
Past medical history revealed that 2 months earlier he was referred to another facility after a BAT due to a car accident. Computed tomography (CT) scan revealed an AAST Grade 2 liver laceration with a small amount of free fluid in Douglas’s pouch. Non operative management was established, and the patient was discharged after 5 days. One month after trauma, he returned to the same hospital suffering from SBO with severe acute kidney injury. The CT scan showed a not otherwise specified thickening of an ileal loop. The SBO was successfully managed conservatively with oral administration of Gastrografin obtaining prompt resolution of patient conditions that led to a discharge after 10 days of hospital stay.
We submitted the patient to a CT scan demonstrating a 10-cm segment of concentric stenosis involving the distal ileum, associated with wall thickening and mesenteric hyperemia, suggesting an inflammatory or ischemic process. The proximal whole small bowel was markedly dilated (Fig. 1).
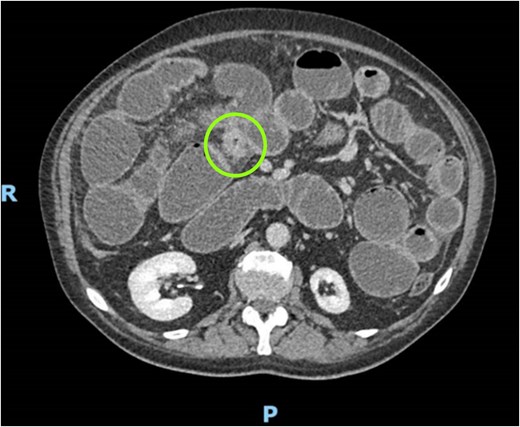
CT scan demonstrating concentric stenosis (circle) and dilated small bowel.
Given the past medical history, the recurrence of the SBO, and the inconclusive imaging findings, an exploratory laparotomy was undertaken. A 4-cm circumferential thickening of the ileal wall was identified at the transition point between dilated proximal and collapsed distal bowel loops. The adjacent mesentery showed evidence of laceration and multiple foci of steatonecrosis (Fig. 2). Ileal resection was performed and intestinal continuity was restored through a hand-sewn, side-to-side isoperistaltic ileal anastomosis. Furthermore, a cirrhotic liver was observed.

Intraoperative findings.
Histopathological examination of the resected specimen documented intestinal mucosa with inflammatory exudate, necrosis, ulceration, and granulation tissue extending into sub mucosae. It was also present hemorrhage, edema, and mesenteric steatonecrosis (Fig. 3). Although the postoperative course was characterized by an elevation of alanine aminotransferase (ALT), aspartate aminotransferase (AST) and INR, the patient gradually resumed normal bowel function and oral feeding and was discharged on postoperative Day 8 in good general condition.
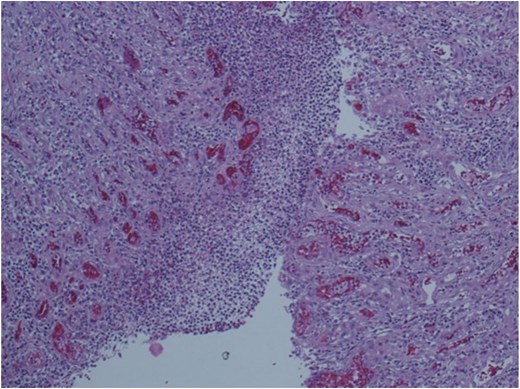
Histopathological examination of the resected specimen.
Discussion
In BAT, hollow viscus and mesenteric injuries account for ~10% of intra-abdominal lesions [3]. Although less common than solid organ injuries, such lesions carry significant diagnostic and therapeutic challenges due to their subtle or delayed clinical presentation [4]. Mesenteric injuries encompass a broad spectrum of pathological findings ranging from minor contusions and localized hematomas to partial lacerations, or, in severe cases, to complete avulsion [5, 6]. Any detachment or segmental tear can lead to devascularization of the bowel, producing ischemia or transmural necrosis or secondary perforation. The clinical presentation of mesenteric injury can vary from acute to chronic. Acute symptoms may be absent or nonspecific in the initial hours following trauma [2]. Radiological assessment plays a pivotal role in these scenarios. However, early radiological evaluation can occasionally fail to detect the full extent of injury, leading to underdiagnosis at the time of index emergency admission [7]. Consequently, a proportion of patients may present delayed complications, including intestinal obstruction secondary to hematoma, adhesive band formation, internal hernia, and ischemic stricture even mimicking inflammatory bowel disease [8].
Our case entails a delayed complication of mesenteric injury where the core feature is the uncommon presentation in which the SBO occurred. In most cases of mesenteric ruptures, in fact, it can happen that we are faced with an internal hernia through the defect because the tear creates a hole, the so called bucket-handle mesenteric tears [9] into which the intestinal loops can slip. Our case doesn’t have any internal hernia but rather a “sleeved” fibrotic reaction which caused the subsequent obstruction. By searching in literature, similar cases can be found. Northcutt et al. [10] analyzed a case of a patient who, following BAT, presents a mesenteric hematoma, treated conservatively, which worsened in the following 2 weeks in an intestinal obstruction. Chatzis et al. [11] reported a case in which a patient was hospitalized multiple times for nausea and vomiting and was always treated conservatively. Furthermore, Gun Hi Kang et al. [12] described a case in which 3 months after trauma a patient presents an ileal stenosis due to a thickening of the intestinal wall.
These diagnostic challenges underline the need for a high index of suspicion in all patients with BAT and unexplained abdominal symptoms. Prompt recognition and appropriate surgical intervention remain essential to minimize morbidity and mortality associated with delayed diagnosis of mesenteric trauma. Although the CT scan should be considered as a gold-standard diagnostic tool [13], a point of care ultrasound can be sometimes helpful [14].
This case highlights that in patients with a history of BAT and evolving gastrointestinal symptoms, clinicians should maintain a high index of suspicion for post-traumatic mesenteric complications. Early recognition and timely surgical intervention are pivotal to prevent irreversible damage and improve clinical outcomes.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}