





Abstract
Mortality and morbidity following pancreaticoduodenectomy (PD) have significantly decreased due to multimodal treatment approach and refinement in surgical techniques. Despite lacking proven benefits, surgeons continue using pancreaticojejunostomy (PJ) transanastomotic stent to mitigate post-operative pancreatic fistula (POPF). We share a morbid case of jejunal perforation caused by PJ stent. A 69 years male presented with features of gastric outlet obstruction secondary to carcinoma second part of duodenum. After proper optimization, he underwent pylorus resecting PD with child’s reconstruction and placement of a transanastomotic PJ stent. Initial postoperative course was well. Later he developed signs of biliary peritonitis. Computed tomography of abdomen revealed perforation of jejunal segment between PJ and hepaticojejunostomy. Despite urgent re-exploration and repair of perforation, the patient ultimately succumbed to sepsis, multi-organ failure, and died. The case highlights the need for thoughtful consideration while attempting to place PJ stents, given the associated risks and the ambiguous impact on mitigating POPF.
Introduction
Mortality and morbidity following pancreaticoduodenectomy (PD) have significantly decreased due to multimodal treatment approach and refinement in surgical techniques. However, despite various mitigation strategies, the rate of post-operative pancreatic fistula (POPF) is still high, and it is a major determinant of post-operative outcomes. The use of an internal pancreaticojejunostomy (PJ) stent is debatable in the literature. Although evidence favouring PJ transanastomotic internal stents is conflicting, many surgeons continue its use in selected cases. Case reports of stent-related complications like stent occlusion and migration, bile duct stricture, stone formation, liver abscess, bowel obstruction, and perforation are increasing [1–7]. We share our experience of a morbid case of jejunal perforation caused by PJ stent.
Case report
A 69-year-old male, reformed smoker and alcohol consumer with no known comorbidities; presented to the emergency department with complaint of non-bilious vomiting for 1 month. It was associated with anorexia and significant weight loss. No history suggestive of GI bleeding.
On examination, patient had grossly normal vital parameters with body mass index (BMI) of 18.84 kg/m2 and Eastern Cooperative Oncology Group performance status grade 2. Abdomen was scaphoid with no features of ascites or jaundice. Patient’s hematological and biochemical parameters were within normal limits with Hb 11.2 gm/dl, serum albumin 3.52 gm/dl, carcinoembryonic antigen (CEA) 0.68 ng/ml, carbohydrate antigen (CA) 19.9–4.31 U/ml. Contrast enhanced computed tomography (CECT) abdomen and pelvis revealed heterogeneously enhancing asymmetrical wall thickening of second part of duodenum causing luminal narrowing with dilatation of first part of duodenum and stomach, dilated common bile duct (CBD) of 10.6 mm diameter with dilated intrahepatic biliary radicals and pancreatic duct diameter of 3 mm. On endoscopy, stomach was distended and filled with food particles with non-negotiable stricture at second part of duodenum. Endoscopic biopsy from the lesion revealed moderately differentiated adenocarcinoma. Patient was initially managed with intra-venous fluids and NG decompression of stomach with parenteral nutritional support. After proper optimization, he underwent pylorus resecting PD with findings of hard mass at peri-ampullary region with soft pancreas and main pancreatic duct (MPD) diameter of 3 mm. Reconstruction was performed using the Child’s technique with modified Blumgart PJ and placement of trans-anastomotic stent (5F infant feeding tube; 15 cm length) with two closed suction abdominal drains (Jackson-Pratt drains) in peri-pancreatic and subhepatic spaces. Patient had normal post-operative course and was tolerating semi-solid diet orally. He developed grade A POPF (Day 3 and Day 5 drain fluid amylase were 1276 and 2307 U/L, respectively) with no change in clinical course till 5th post-operative day (POD). On POD 6, he developed tachycardia and epigastric tenderness with localized guarding and high output bilious drainage along with bilious discharge from wound. CECT abdomen revealed perforation of jejunal segment between PJ and hepaticojejunostomy (HJ) with part of the stent in the localized intra-peritoneal collection (Fig. 1).
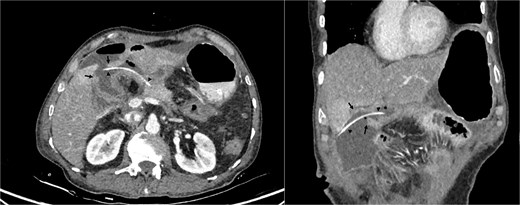
Cross-sectional image of jejunum perforation (black arrows) and transanastomotic pancreaticojejunostomy stent (black arrow heads).
On re-exploration, perforation of 2 × 2 cm noted in the anti-mesenteric border of jejunum with intact PJ and HJ anastomotic sites (Fig. 2). Peritoneal lavage with stent removal and primary repair of jejunal perforation with omental patch re-enforcement was done. Patient was shifted to ICU intubated. He was extubated on the 1st POD of re-exploration. On the 3rd POD, he was again intubated and was started on ionotropic supports for not maintaining saturation and septic shock. Ionotropic supports increased the following day and patient died on 4th POD after re-exploration due to sepsis and multi-organ failure.
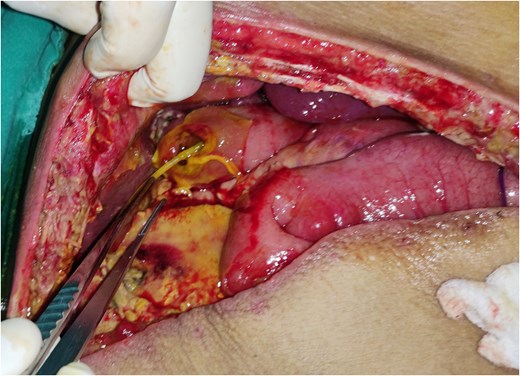
Jejunal perforation defect with stent through the perforation.
Discussion
POPF is a common complication and a major determinant of post-operative outcomes following PD. Pancreatic stents used to mitigate the risk of POPF, are not without risks. Our case presents a rare and dreaded complication of transanastomotic PJ internal stent related jejunum perforation following PD.
Trans-anastomotic PJ stent serves to facilitate for accurate placement of anastomotic sutures and prevent iatrogenic ductal occlusion, especially in cases of small pancreatic duct. It also helps to decompress pancreatic duct while maintaining anastomotic patency and avoid placement of external stents [8]. The literature on pancreatic stenting to mitigate POPF is conflicting [9]. Despite the evidence, surgeons continue its use in selected high-risk cases. The use of external stents, however, is limited by specific complications of early displacement, stent occlusion, peritonitis, abdominal collections, and abscess formation [10]. In our case, internal stent was placed for small MPD size ( ~3 mm diameter) and soft pancreas. The patient initially had uncomplicated postoperative course until 6th POD, then he developed signs of peritonitis and bilious drainage. Cross sectional imaging revealed jejunal perforation and part of stent protruding through the defect. Despite prompt surgical intervention, the patient initially showed signs of improvement following re-exploration but ultimately succumbed to sepsis, multi-organ failure, and died.
The perforation in our case could have likely resulted from direct mechanical trauma by the stent’s rigid tip against the jejunal wall, compounded by the patient’s poor nutritional status (BMI 18.84 kg/m2, prolonged vomiting) and delayed hospital presentation. Similar case reports of stent related jejunum perforation occurring as early as 36 hours to 19 years following the surgery [3–5, 7] highlights the unpredictable nature of the complication.
This case compelled us to re-consider the decision for stent placement following PJ. To prevent such complications in the future and subsequent cases, we propose to use a single-J stent with the blunt/curved end placed in the jejunum and straight end into the pancreatic duct. In this way there won’t be direct trauma on the jejunal wall (Fig. 3).
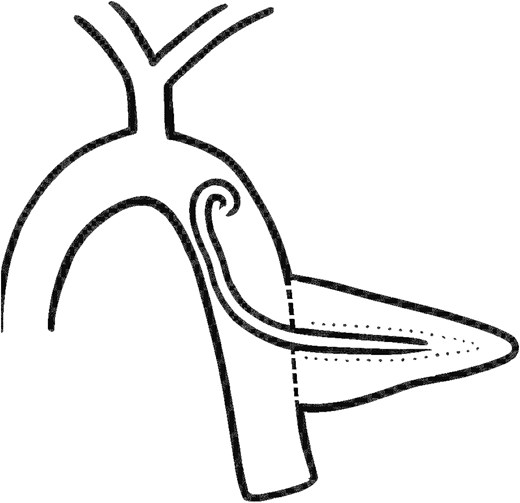
Improvised technique of single-J transanastomotic stent placement.
While internal stents are theorized to reduce POPF rates by decompressing the pancreatic duct and ensuring anastomotic alignment, emerging reports of stent related complications question its actual/overall benefit. A thoughtful consideration is critical on re-assessing their routine use, given the potentially fatal complications associated with it. Future studies should focus on risk stratification to identify patients who may truly benefit from stenting versus those at risk of complications.
Jejunal perforation is a dreadful complication of transanastomotic PJ stent following PD. Thoughtful consideration is essential when attempting to place internal transanastomotic PJ stents, given the associated risks and the ambiguous impact on mitigating POPF.
Acknowledgements
The author thanks the surgical, intensive care and pathology teams for their contributions in patient management.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No specific funding was received for this study.

{kind=link}
{kind=link}
{kind=link}