





Abstract
Follicular unit excision (FUE) is a widely used hair transplantation technique with a favorable safety profile; however, rare but severe complications such as recipient-site scalp necrosis can occur. We report a 46-year-old male with androgenetic alopecia who developed early-onset recipient-site necrosis following FUE hair transplantation. Dusky discoloration appeared on postoperative day two and progressed to extensive necrosis with yellowish crusting by day ten. Wound culture revealed secondary Pseudomonas aeruginosa infection. The patient had a history of heavy smoking and underwent a prolonged nine-hour procedure. Management with conservative wound care and culture-guided systemic antibiotics led to resolution of infection, with healing resulting in residual atrophic cicatricial scarring at 12 weeks. This case highlights that recipient-site necrosis, although rare, may arise from the synergistic effects of patient-related risk factors, prolonged operative duration, dense graft placement, and secondary infection. Early recognition and prompt intervention are critical to minimizing tissue loss and optimizing outcomes.
Introduction
Follicular unit excision (FUE) has become one of the most widely used techniques for surgical hair restoration because of its minimally invasive nature and favorable cosmetic outcomes [1]. With its increasing popularity, a parallel rise in procedure-related complications has been observed [2]. Commonly reported complications include scarring, folliculitis, infection, bleeding, edema, neuralgia, pruritus, and post-inflammatory pigmentary changes [2]. Less frequently reported adverse events include pyogenic granuloma, arteriovenous fistula, herpes zoster, malignant hyperthermia, lichen planopilaris, post-traumatic neuroma, and trichorrhexis nodosa [2, 3].
Among these complications, scalp necrosis is particularly rare but potentially devastating [3]. Beyond compromising graft survival, it may result in irreversible tissue loss and can progress to severe complications such as deep soft-tissue infection or cranial osteomyelitis [4].
Herein, we report a case of early-onset recipient-site necrosis following FUE, complicated by secondary Pseudomonas aeruginosa infection.
Case presentation
A 46-year-old male with androgenetic alopecia (AGA) presented to our dermatology clinic with yellowish crusting and extensive necrosis involving the frontal scalp. Ten days earlier, he had undergone FUE hair transplantation at a private hair transplant center. The patient reported the development of dusky discoloration in the recipient area on postoperative day 2 (Fig. 1).
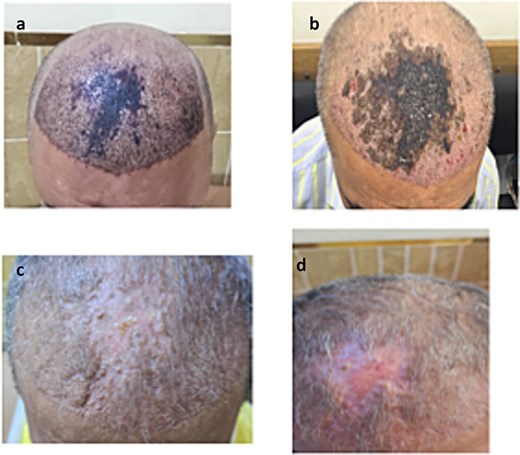
Clinical progression of recipient-site necrosis following follicular unit extraction (FUE). (a). Early postoperative dusky violaceous discoloration of the central frontal scalp, suggestive of impending ischemia. (b). Development of yellowish crusting and extensive necrosis involving the central frontal region. (c). Following systemic antibiotics and daily conservative wound care, crust resolution with formation of early atropic scar. (d). 12-week follow-up showing complete epithelialization of the necrotic recipient site, resulting in a stable atrophic scar with telangiectasia and permanent alopecia confined to the affected area.
He was diagnosed with recipient-site scalp necrosis complicated by secondary infection and was initially treated with daily wound care, oral cefdinir 400 mg twice daily, and topical mupirocin. A wound culture subsequently grew P. aeruginosa. Based on culture and sensitivity results, systemic therapy was switched to oral ciprofloxacin, resulting in gradual clinical improvement and resolution of the infection.
At the 12-week follow-up visit, the eschar had separated spontaneously, leaving an atrophic cicatricial scar in the central frontal scalp.
Regarding surgical details, the patient stated that the FUE procedure lasted ~9 h; however, he was unable to recall the number of grafts implanted. His medical history was significant for heavy tobacco use, smoking approximately three packs per day.
Discussion
Recipient-site necrosis is an uncommon but serious complication of hair transplantation that can result in significant esthetic deformity, particularly when the central scalp is involved—an area with relatively reduced vascularity [1, 2, 5]. Early recognition and prompt intervention are essential to limit tissue loss and graft failure.
The fundamental mechanism underlying scalp necrosis is insufficient perfusion of the recipient area. Several contributing factors have been described [2, 6, 7]:
Reduced baseline scalp vascularity in AGA
Heavy smoking, as in our case, which induces vasoconstriction, impairs endothelial function, and compromises microcirculation
Dense graft placement, particularly at densities exceeding 50 follicular units/cm2
Excessive use of vasoconstrictive agents, especially high-dose epinephrine
Prolonged operative duration with cumulative tissue trauma
In this patient, the combination of heavy smoking, a prolonged nine-hour procedure, and probable dense graft packing with epinephrine infiltration likely created a profoundly ischemic environment. Secondary P. aeruginosa infection further exacerbated tissue injury and necrosis [6]. This sequence—primary ischemia followed by opportunistic bacterial colonization—is well recognized in necrotic surgical wounds.
Although vascular injury associated with FUE is generally minimal, dense graft placement in a hypoperfused recipient bed significantly increases the risk of necrosis [7]. Following infection control and gradual revascularization via collateral circulation, healing may occur; however, permanent atrophic scarring is common, as observed in our case. This underscores the importance of meticulous preoperative risk stratification, particularly in high-risk patients such as heavy smokers.
Conclusion
Despite its minimally invasive nature, FUE hair transplantation can be associated with rare but severe complications such as recipient-site scalp necrosis. This case highlights the critical role of patient-related risk factors especially heavy smoking along with careful intraoperative planning and early recognition of ischemic changes. Increased awareness of this potentially devastating complication may help clinicians reduce tissue loss, optimize wound healing, and improve overall surgical outcomes.
Conflict of interest
There is no conflict of interest to report.
Funding
No source of funding was received.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Ethics approval
Our institution does not require ethical approval to report individual cases or case series.

{kind=link}