





Abstract
A 40-year-old lady with a known history of gallstones presented with acute abdominal pain. Diagnostic imaging confirmed cholelithiasis with concomitant choledocholithiasis. She underwent a therapeutic endoscopic retrograde cholangiopancreatography for stone extraction. Her post-procedural course was complicated by the development of severe acute pancreatitis. Despite aggressive medical management, her clinical condition deteriorated rapidly. Subsequent computed tomography scans revealed extensive pancreatic necrosis and a perforation of the splenic flexure of the colon. The patient was taken for emergency surgery. An exploratory laparotomy was performed. Resection of the affected splenic flexure, a primary anastomosis, and the creation of a proximal loop ileostomy done. The patient recovered without further major complications. She was discharged in satisfactory condition with plans for ileostomy reversal later on. This case underscores the dictum that in medicine, a benign-looking pathology can have malignant consequences, demanding respect, timely intervention, and relentless monitoring.
Introduction
Cholelithiasis or gallstone disease, affects a significant portion of the adult population. While often asymptomatic, it can lead to severe complications such as acute cholecystitis, cholangitis, and pancreatitis if untreated [1].
Endoscopic retrograde cholangiopancreatography (ERCP) is a widely used minimally invasive procedure for diagnosing and treating Choledocholithiasis, the presence of gallstones in the common bile duct (CBD) [2].
A well-documented complication of ERCP is post-ERCP pancreatitis, occurring in 3%–10% of cases. Most cases are mild and self-limiting. However, a small subset of patients develops severe, necrotizing pancreatitis, which carries substantial morbidity and mortality. Colonic complications of severe pancreatitis including ischemia, fistula formation, and perforation are rare but catastrophic, resulting from the direct enzymatic action of pancreatic exudates and local vascular compromise [2].
This case report describes a rare escalation of events in a 40-year-old lady where post-ERCP severe acute pancreatitis resulted in colonic perforation, necessitating emergency surgery. It serves as a cautionary example of how seemingly ‘simple’ gallstones can become life-threatening if ignored or if procedural complications arise, emphasizing the need for early intervention and vigilant monitoring.
Case report
A 40-year lady presented to emergency with complaints of severe pain abdomen and vomiting. She was already diagnosed case of symptomatic cholelithiasis with choledocholithiasis at an outside facility, for which endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy with pancreatic duct (PD) and CBD stenting was done 10 days back. Since her clinical condition was not improving. So, she presented to our hospital for more intensive treatment.
Examination
On presentation her vitals were temperature 38.0°C, heart rate 122 bpm, respiratory rate 26, blood pressure 104/62 mm Hg @ Norad 4 ml/hr, and oxygen saturation 91% on room air. She was in acute distress. Abdominal examination showed distended abdomen, diffuse tenderness without rigidity and decreased bowel sounds.
Laboratory tests
Haemoglobin 9.2 g/dl; WBC 17200 cells/mm3 (neutrophils 75.3%); AST 118 IU/L; ALT 123 IU/L; alkaline phosphatase 231 IU/L; total bilirubin 0.5 mg/dl; serum amylase 817 U/L; serum lipase 1840 U/L; and serum lactate 3.9 mmol/L, blood urea nitrogen 26 mg/dl, creatinine 1.9 mg/dl.
Imaging
As shown in Fig. 1, computed tomography (CT) scan of abdomen showed pneumoperitoneum in inter bowel space, pancreatic necrosis, peripancreatic collection in splenic flexure region with multiple air foci within it and adjacent mesenteric fat stranding and heterogeneity. (? Splenic flexure of Colon perforation).
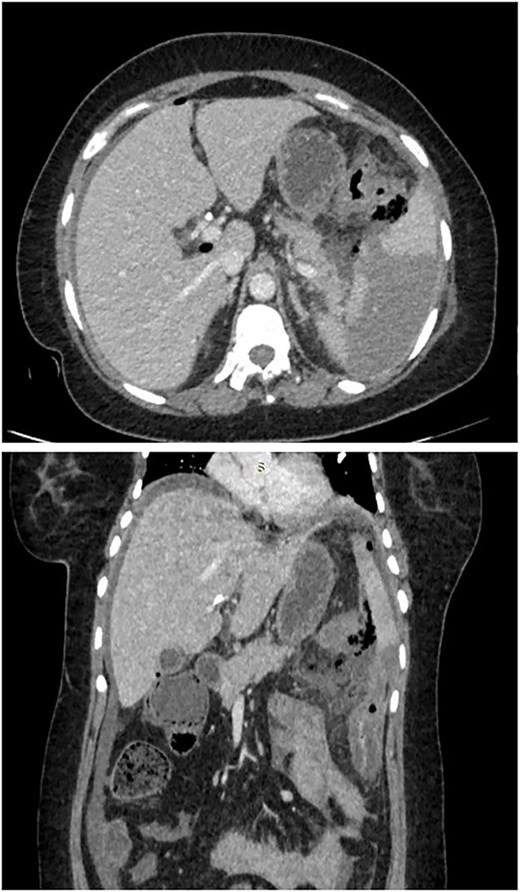
CT scan of abdomen showed pneumoperitoneum in inter bowel space, pancreatic necrosis, peripancreatic collection in splenic flexure region with multiple air foci within it and adjacent mesenteric fat stranding and heterogeneity. (? Splenic flexure of colon perforation).
Management
Patient was taken for emergency laparotomy which showed ~200 ml of pancreatic free fluid with purulent and feculent material, calcified pancreas with dense adhesions, 2 × 1 cm perforation in splenic flexure of colon as shown in Fig. 2. Resection and anastomosis of splenic flexure of colon with proximal loop ileostomy with placement of 2 abdominal drain was done. Patient was shifted to intensive care unit for post op care.
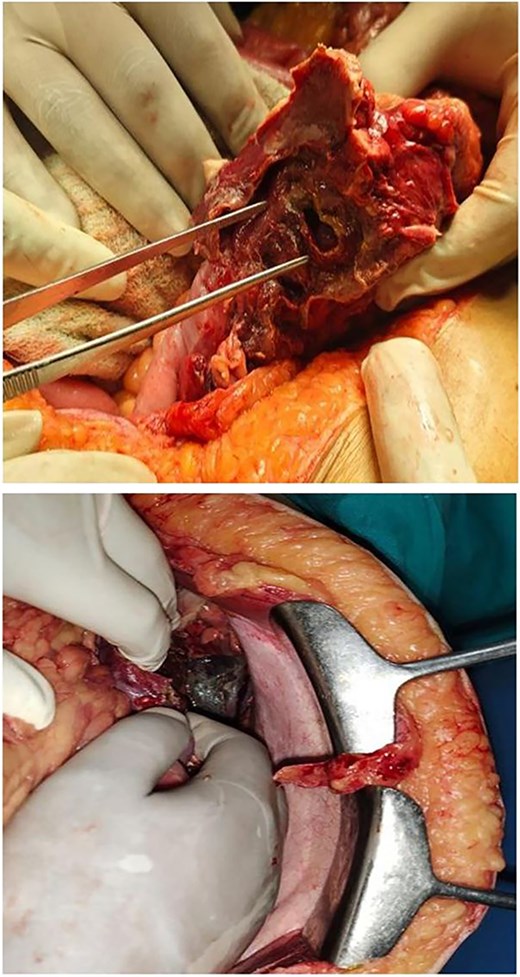
2 × 1 cm splenic flexure of colon perforation & necrotic pancreas.
Outcome
The post op period was uneventful. Patient was discharged in stable condition after 2 weeks of hospital stay. She continued to follow-up in the outpatient department and is currently doing well. Now, she is planned for ileostomy closure soon.
Discussion
Colonic complications are observed in up to 10% of patients diagnosed with severe acute pancreatitis and include ileus, abscess, obstruction, fistula, and perforation [3]. Colonic perforation is an infrequent medical event, and as such, the available literature consists primarily of case studies.
The patient in this report experienced a perforation at the splenic flexure of colon and it is also the most common site. The mechanism of colonic perforation in acute pancreatitis is multifactorial. The close anatomical relationship between the pancreatic tail and the splenic flexure of the colon makes it vulnerable. The release of proteolytic pancreatic enzymes can lead to direct digestion of the colonic wall. Furthermore, the intense inflammatory response can cause thrombosis of mesenteric vessels, leading to ischemic necrosis and subsequent perforation. The splenic flexure is particularly susceptible due to its watershed blood supply [4].
Research from Nakanishi et al. provides some of the limited data, indicating a 5.3% incidence of colon perforation with a median onset of 13 days following the start of symptoms. The timing of this patient's colonic perforation, at 10 days after the initial symptoms of acute pancreatitis, is consistent with the median onset time observed in other reported cases [5].
The mortality rate for severe acute pancreatitis can be as high as 30%. When surgical treatment is required, this risk escalates to ~40% because of the additional stress. As described in Table 1, similar mortality reported in many cases by Liew [3], Nagpal [4], and Nisserine et al. [6].
Summary of major studies on colonic perforation with pancreatitis
| Author / Year | Age / Sex | Site | Cause of pancreatitis | Procedure | Outcome |
|---|---|---|---|---|---|
| Liew et al., 2025 [3] | 61y/ Female | Caecum | Idiopathic | Exploratory laparotomy and oversown perforation | Uneventful |
| 72y/ Male | Sigmoid colon | Gallstones | Total colectomy | Uneventful | |
| Nissrine et al., 2025 [6] | 38y / Male | Transverse colon | Gallstones | Exploratory laparotomy | Intraoperative death |
| Saleh et al., 2024 [7] | 60y / Female | Sigmoid colon | Idiopathic | Exploratory laparotomy with diversion colostomy | Uneventful |
| Hozaka et al., 2019 [8] | 31y / Male | Splenic flexure of colon | Gallstones | Video-assisted retroperitoneal debridement with proximal loop ileostomy | Uneventful |
| Dhadlie et al., 2019 [9] | 70y / Male | Ascending colon | Gallstones | Exploratory laparotomy with right sided hemicolectomy with end ileostomy | Uneventful |
| Nagpal et al., 2015 [4] | 35 y / Male | Splenic flexure of colon | Gallstones | Exploratory laparotomy with subtotal colectomy with proximal loop Ileostomy | Uneventful |
| 54y / Male | Transverse colon | Gallstones | Exploratory laparotomy with subtotal colectomy with proximal loop Ileostomy | Death in post operative period | |
| Naidoo et al., 2014 [2] | 41y / Female | Transverse colon | Post ERCP | Extended right hemicolectomy with end-ileostomy | Uneventful |
These patients are often septic, even when receiving the highest level of conservative care, indicating a need for urgent surgical management. Source control through colonic resection and damage control surgery is crucial for immediate sepsis resolution [3]. Furthermore, to reduce the risk of anastomotic leaks, a diverting loop ileostomy is recommended if an anastomosis is performed, as it reduces the overall hospital stay and mortality. Similar result found in our case, 2 weeks stay as compared to longer stay (1 month – 3 month) in other reports [4].
Conclusion
Neglected symptomatic gallstone disease is not benign. It can set off a cascade of severe, life-threatening complications. This case report serves as a stark reminder that severe post-ERCP pancreatitis can lead to rare but devastating extra pancreatic consequences like colonic perforation. It emphasizes the importance of timely cholecystectomy in patients with symptomatic gallstones to prevent the need for higher-risk procedures and their potential complications. This case underscores the dictum that in medicine, a benign-looking pathology can have malignant consequences, demanding respect, timely intervention, and relentless monitoring.
Conflicts of interest
No conflict of interest exists in the submission of this manuscript, and the manuscript has been approved by all authors for publication.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.

{kind=link}
{kind=link}