





Abstract
This case report describes a high-grade recurrent aortic coarctation incidentally detected in a 7-year, 10-month-old girl, seven years after primary balloon dilatation. Echocardiography identified narrowing of the descending aortic arch. Computed tomography of the chest with three-dimensional reconstruction further delineated severe focal stenosis at the aortic isthmus, adjacent to the left subclavian artery origin, with a minimal luminal diameter of 0.5 cm. Post-stenotic dilation of the proximal descending aorta measured up to 2.7 cm. The patient underwent successful surgical repair with artificial vascular bypass under extracorporeal circulation. Postoperative imaging confirmed graft patency. Symptoms resolved after surgery, and the patient continues under long-term follow-up. This case highlights the risk of delayed, severe recoarctation after balloon angioplasty and emphasizes the importance of sustained imaging surveillance in these patients.
Introduction
Coarctation of the aorta is a congenital aortic malformation that occurs in the narrowed or stenotic area from the ascending aorta to the descending aorta and distal to the connection between the aorta and the ductus arteriosus, with a prevalence of ~5%–8% [1, 2], whereas recurrence after intervention and close to the aorta and left subclavian children is rare, we report such a case of incidental recurrence of high coarctation of the aorta in a child.
Case report
Female, 7 years old and 10 months old, 7 years after aortic balloon dilatation, echocardiography showed a narrow internal diameter of the descending aortic arch (Fig. 1A, arrows), computed tomography (CT) of the chest showed that the aortic isthmus was narrowed in close proximity to the left subclavian artery (Fig. 1C, arrowheads), and three-dimensional (3D) reconstruction showed that the isthmus of the aorta was significantly stenosed locally, with a ductal diameter of ~0.5 cm, and the proximal descending aorta in the proximal part of the aorta was thickened, with a maximal ductal diameter of ~2.7 cm, and the narrowing part was close to the left subclavian artery (Fig. 1B, arrow). The operation was performed by artificial vascular bypass grafting under extracorporeal circulation, and the 3D reconstruction showed that the bypass grafting was successful (Fig. 1D, arrow), and the child's symptoms were relieved after the operation, and the child was followed up for a long period of time.
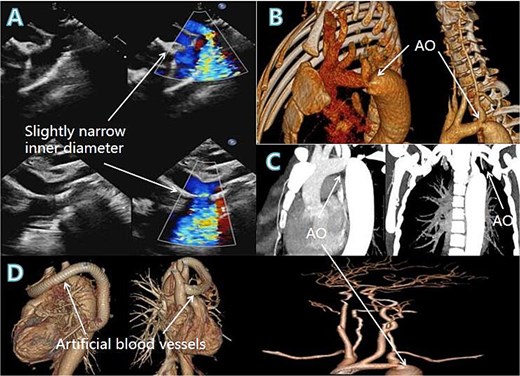
Coloured blood flow signals from the descending aortic arch (A, arrow), 3D reconstruction and chest CT showing the area of aortic stenosis (B, C, arrows), postoperative 3D reconstruction showing the artificial vessel and the success of the procedure (D, arrow).
Discussion
Balloon dilatation was performed in childhood to treat high coarctation of the aorta, and after many years of high incidental recurrence, and the location is very close to the left subclavian artery, and coupled with age limitations, the advantages of artificial vessel bypass grafting are particularly prominent at this time, in order to relieve the high pressure caused by coarctation of the aorta, but also to minimize the harm to the child, and such a case is very rare. Currently, the main treatment for coarctation of the aorta is surgery, which includes resection of the constricted segment with end-to-end anastomosis or artificial vascular grafting, coarctation of the aorta angioplasty, coarctation of the aorta artificial vascular bypass grafting, and interventional treatments such as simple balloon dilatation, aortic stenting, and can be used for some simple and limited coarctation of the aorta in adults as well as infantile coarctation of the aorta [3, 4].
Conclusion
The choice of procedure varies greatly depending on the location of the constriction, the variability of the vessel, and the patient's own condition, and CT angiography can be helpful in the diagnosis and treatment of this disease.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
No funding was received for this work.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
References
Stephens EH, Feins EN, Karamlou T et al. The Society of Thoracic Surgeons clinical practice guidelines on the management of neonates and infants with coarctation. The Annals of Thoracic Surgery 2024;118:527–44.

{kind=link}