





Abstract
Melorheostosis is a progressive sclerosing bone dysplasia that rarely involves the spine. When spinal involvement occurs, it can lead to significant neurological compromise due to spinal cord compression. We report the case of a previously healthy 22-year-old woman who presented with progressive gait instability and upper motor neuron symptoms secondary to a hyperostotic lesion extending from C2 to C5. Imaging demonstrated severe left-sided spinal canal stenosis, prompting urgent surgical decompression with posterior cervical fusion. Intraoperative neuromonitoring showed complete loss of all sensory and motor potentials from the left side following decompression. Accordingly, she woke up with complete hemiplegia; however, rapid improvement was noted over the following days. Through analysis of 25 documented cases, we highlight the variability in anatomical involvement, clinical presentation, and management strategies. This report underscores the importance of an individually tailored surgical intervention and contributes to the scarce literature on cervical spinal melorheostosis.
Introduction
Melorheostosis, first described by Leri and Joanny in 1922 [1], is a rare, benign sclerosing bone dysplasia with an estimated incidence of 0.9 cases per million individuals [2]. It is characterized by the development of dense cortical hyperostosis following a sclerotomal distribution. Although its exact pathophysiology remains unclear, somatic mutations in the MAP2K1 gene have recently been implicated in its development [2].
Radiographically, the hallmark appearance resembles “dripping candle wax” along the surface of affected bones. While the disease most commonly involves the appendicular skeleton, axial involvement is distinctly uncommon. Spinal manifestations are exceedingly rare, with only a limited number of cases reported. When present, spinal melorheostosis may result in significant neurological compromise due to compressive myelopathy or radiculopathy [3–5], often requiring surgical intervention.
In this report, we present a rare case of cervical spinal melorheostosis leading to severe spinal cord compression and progressive neurological decline. We describe the clinical course, radiographic features, surgical management, and histopathological findings, alongside a review of the existing literature.
Case report
Clinical presentation
A 22-year-old woman with no significant past medical history presented with a 6-month history of progressive gait instability and clumsiness of the left hand. She reported increasing difficulty with fine motor tasks and intermittent axial neck pain, accompanied by subjective upper extremity (UE) weakness. Neurological examination revealed hyperreflexia, positive Babinski sign on the left, and impaired proprioception in the left UE and lower extremity (LE). Motor strength was reduced to grade 4−/5 in the affected limbs.
Imaging findings
Magnetic resonance imaging (MRI) of the cervical spine demonstrated a hyperostotic lesion extending from C2 to C5. The lesion appeared predominantly intraosseous with periosteal extension but without involvement of adjacent soft tissues. There was significant left-sided spinal canal encroachment, resulting in severe cord compression (canal narrowing <5 mm). T2-weighted sequences showed deformation and signal changes within the spinal cord consistent with compressive myelopathy (Fig. 1). Complementary computed tomography (CT) revealed dense cortical hyperostosis with a characteristic “dripping candle wax” appearance (Fig. 2).
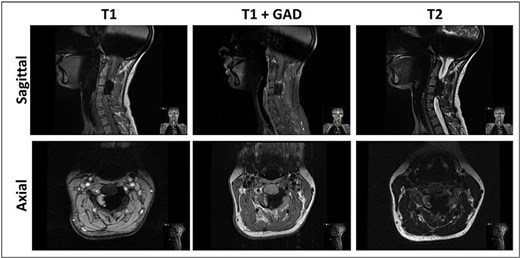
MRI sagittal and axial views of the cervical spine demonstrating non-enhancing, hypointense in all sequences, calcified lesion involving mainly C3–C4, causing severe compression of the spinal cord with hyperintense signal, indicating myelomalacia.
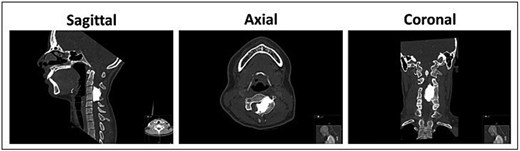
Pre-operative CT scan of the cervical spine demonstrating dense cortical hyperostotic lesion along the anterior and posterior elements of C3–C4 with classic “dripping candle wax” morphology, indicative of melorheostosis.
Surgical management
Radiological findings, combined with progressive clinical deterioration, prompted surgical intervention. The patient was positioned prone on a Jackson table (using a “Jackson flip” maneuver), with the head immobilized in a Mayfield three-pin skull clamp. Baseline motor and somatosensory evoked potentials were established.
A posterior cervical approach was performed, comprising a wide C3–C4 laminectomy and partial decompression of C2 and C5. The decompression extended anterolaterally to access the ventral aspect of the C3 vertebral body. Intraoperatively, a dense sclerotic lesion was identified compressing the dorsal spinal cord and displacing the left vertebral artery. To mitigate the risk of vascular injury, a near-total resection was performed, intentionally leaving a residual cuff of tumor adherent to the vertebral artery at the C3 level. The final intraoperative scan showed the spinal canal was widely decompressed and cleared of the bony mass, with only a thin residual cuff remaining.
Stabilization was achieved via posterior fixation using bilateral C2 pedicle screws and C3–C5 lateral mass screws connected by rods. Decortication was performed, and an allograft was applied to promote fusion. Following decompression, neuromonitoring detected a complete loss of left-sided Motor evoked potentials (MEPs) and Somato-sentory evoked potentials (SSEPs). However, microscopic inspection revealed no mechanical trauma or dural tear. Adequate decompression and hardware placement were confirmed via intraoperative CT (Fig. 3).
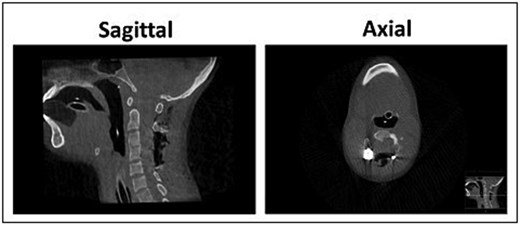
Post-operative CT scan of the cervical spine demonstrating post-operative adequate decompression and alignment, with canal dimensions increasing from a minimal preoperative size of 4.7 × 12.1 mm (Anterior-Posterior*BiLateral) to 27.3 × 17.7 mm at the level of upper 1/4 of C4.
Postoperative course
The immediate postoperative period was marked by transient worsening of left-sided hemiparesis. However, the patient demonstrated rapid neurological improvement within days. At discharge, she had mild residual paresis and proprioceptive deficits confined primarily to the proximal muscles of the left UE. By the first follow-up visit six weeks later, only mild (4+/5) proximal left UE paresis was noted.
Discussion
Melorheostosis is a benign sclerosing bone dysplasia characterized by abnormal proliferation of cortical bone. Although histologically benign, it can behave aggressively in the axial skeleton, leading to neurologic compromise and structural instability. In most cases, the disease remains indolent; however, progression following incomplete surgical excision [6] and, in exceedingly rare instances, malignant transformation [7] have been documented.
To contextualize this case, we analyzed 25 cases [8–10] of spinal melorheostosis identified in the literature (Table 1). The mean patient age was 38 years, with a nearly equal sex distribution. The thoracic spine was the most frequently affected region (15 cases), followed by the cervical (10 cases) and lumbosacral (7 cases) segments. Neurological symptoms, including radiculopathy and myelopathy, were common [3, 11]. Notably, five cases reported concurrent lipomatous lesions [12–14], suggesting a possible developmental association.
Summary of 25 reported cases of spinal melorheostosis. Details include year of publication, patient age and sex, spinal involvement, clinical presentation, and treatment approach. The diversity of anatomical locations and treatment strategies highlights the variability of this rare entity
| Number | Year | Age | Sex | Location | Examination and complain | Treatment | Notes |
|---|---|---|---|---|---|---|---|
| 1 | 1982 | 21 | M | Thoraco-lumbar | Quadriparesis; UE + LE weakness | Spinal biopsy | Cervical lipoma |
| 2 | 1988 | 31 | M | Cervico-thoracic | Muscle wasting left leg, UMN, hypoesthesia below T3; Left side limp | Vertebral biopsy | Intradural lipoma |
| 3 | 2001 | 28 | F | T5, L3–S1 | normal:none | Non- not proven | |
| 4 | 2001 | 42 | F | T11–T12 | Paraparesis,T12 sensory level; leg weakness, urinary incontinence | Decompression | Second surgery due to progression |
| 5 | 2003 | 54 | F | L2,3,5 | Normal; low back pain | Decompression + L5–S1 fixation | |
| 6 | 2004 | 40 | F | T10–T11 | Normal, dorsal lump; Back pain | Open biopsy | Subcutaneous necrotic fibrocartilaginous mass |
| 7 | 2004 | 74 | F | C5 | Deltoid atrophy, C5–C6 rediculopathy; Neck and shoulder pain | Non- not proven | |
| 8 | 2005 | 35 | M | Thoracic spine | Shuffling gait, paraparesis – distal worse, hyperreflexia, Babinsky+, ankle clonus; paraparesis, gait abnormality | Cervicothoracic decompressive laminectomy | |
| 9 | 2005 | 35 | M | C5–T4 | Paraparesis 4/5 BLT LE; Cervico-thoracic pain, parapresis, urinary urgency | C5–T4 decompressive laminectomy | |
| 10 | 2006 | 46 | M | C5–T1 | Stiffness; neck pain | Non- not proven | |
| 11 | 2006 | 70 | F | C6–T1 | Normal; cervicobrachialgia | Rt hemilaminectomy C7 | Cervical lipoma |
| 12 | 2009 | 42 | M | T9–11 | Normal; asymptomatic incidental finding | Non- not proven | Suspected RCC metastasis |
| 13 | 2011 | 57 | M | L5-S2 | S1 radiculopathy. Numbness along right leg, neuropathic pain S1 dermatome; back pain radiating to right leg + numbness and weakness | L5 laminectomy and Rt. foraminotomy | |
| 14 | 2013 | 33 | F | L4–L5 | Lt. Quad wasting, hypoesthesia L4 dermatome, Lt. quad hyporeflexia; Left L4–L5 radiculopathy | L4 laminectomy & medial facetectomy L4–L5 | |
| 15 | 2014 | 18 | M | Cervico-thoracic spine | Normal; gait instability + Lt. neck and shoulder pain | Non- not proven | Refused surgery |
| 16 | 2015 | 70 | M | Cervico-thoracic | Normal; asymptomatic incidental finding | Non- not proven | Mostly ribs involvement |
| 17 | 2020 | 33 | M | C1–C2 | Normal; asymptomatic incidental finding | Non- not proven | |
| 18 | 2020 | 33 | M | T11 + rib | Normal; asymptomatic incidental finding | Non- not proven | Extensive disease, multiple bones involvement |
| 19 | 2020 | 22 | F | T8–T9 | Normal; LUQ abdominal radiating pain – T9 radiculopathy | T9 Laminectomy + T8–T10 fusion | |
| 20 | 2022 | 18 | M | Toraco-lumbar | Gait abnormality, LE UMN; radiculopathy, sensory disturbance | Surgery decompression + fusion | Extensive disease, multiple bones involvement |
| 21 | 2022 | 41 | F | T10–T11 | normal:none | Non- not proven | |
| 22 | 2023 | 22 | F | T6 | Normal; none | Open biopsy | |
| 23 | 2024 | 43 | F | C1 | Normal; neck pain | Resection + occiput-C4 fixation w/ bone graft | |
| 24 | 2024 | 23 | F | C2–C4 | Normal; neck pain | Resection + ant. ACF C3–C4 + bone graft and post. Temp. C1–C6 fixation | Cervical lipoma |
| 25 | 2024 | 20 | M | T1–T3 | Normal; cervico-thoracic pain | Non- not proven |
Management strategies varied significantly. Ten patients were treated conservatively, while the remainder underwent surgical decompression due to neurologic deterioration. Our review suggests that surgical indications generally parallel those for degenerative spinal pathologies: refractory pain, progressive neurological deficits, or deformity. Surgical goals include histopathologic diagnosis, decompression of neurovascular structures, and restoration of stability. Posterior approaches are most common, though anterior approaches may be required for ventral disease.
Conclusions
Given the rarity of this condition, a multidisciplinary approach involving spine surgeons, radiologists, and pathologists is essential. Long-term follow-up with serial imaging is recommended to monitor for recurrence, particularly following incomplete resection [15].
Author contributions
NT: data mining, writing. RGY: editing, structure. SH: supervision
Conflicts of interest
The authors declare no conflicts of interest.
Funding
All authors declare no funding was received for this project.

{kind=link}
{kind=link}
{kind=link}