





Abstract
Gallbladder torsion is a rare and severe abdominal emergency with non-specific clinical manifestations. An 82-year-old female patient was initially suspected of having gallstones preoperatively but was subsequently diagnosed with gallbladder torsion postoperatively. This case underscores the critical importance of accurate image interpretation and timely surgical intervention.
Introduction
The phenomenon of gallbladder torsion was initially reported by Wendel in 1898 [1]. The identification of gallbladder torsion in the clinical setting of acute abdominal pain is rare, with fewer than 700 cases reported in the literature to date [2]. Published studies suggest a higher prevalence in both elderly and pediatric populations, with a marked female preponderance in the elderly. The clinical presentation of gallbladder torsion is often non-specific and confused with other etiologies causing acute abdominal pain. Currently, the preoperative diagnosis rate based on clinical presentation and advanced imaging examinations ranges from 10% to 26%, with the vast majority of cases still being definitely diagnosed intraoperatively [3, 4]. This study aims to report a case of gallbladder torsion in an elderly female, where preoperative imaging suggested a neck stone in the gallbladder, but intraoperative diagnosis revealed gallbladder torsion without gallstones.
Case report
An 82-year-old female presented to the emergency department with a 2-day history of right upper quadrant pain accompanied by nausea and vomiting. The patient was hunched and thin, with a body mass index of 15.0 kg/m2 (Fig. 1). Physical examination revealed abdominal tenderness and a positive Murphy’s sign. Routine blood examination showed a white blood cell count of 16.5 × 10 [5], C-reactive protein of 3.83 mg/L, and normal liver function and electrolytes. A non-contrast abdominal computed tomography (CT) scan (Fig. 2) and gallbladder US (Fig. 3) were performed. We administered analgesics and antibiotics for 24 hours based on US and CT findings indicating impacted stones in the neck of the gallbladder. However, the patient’s symptoms of persistent abdominal pain did not improve, prompting us to proceed with laparoscopic exploration. During the operation, a necrotic gallbladder was identified within the confined space of the abdominal cavity (Fig. 3). Subsequently, intraoperative puncture decompression of the gallbladder was performed, followed by exploration via manipulation and rotation of the gallbladder using laparoscopic instruments (Fig. 4). The gallbladder was found to be completely mobile and had undergone a 360°clockwise torsion (Fig. 5). We successfully performed a laparoscopic cholecystectomy and pathological examination showed acute gangrenous cholecystitis. The patient was discharged on the fourth postoperative day.
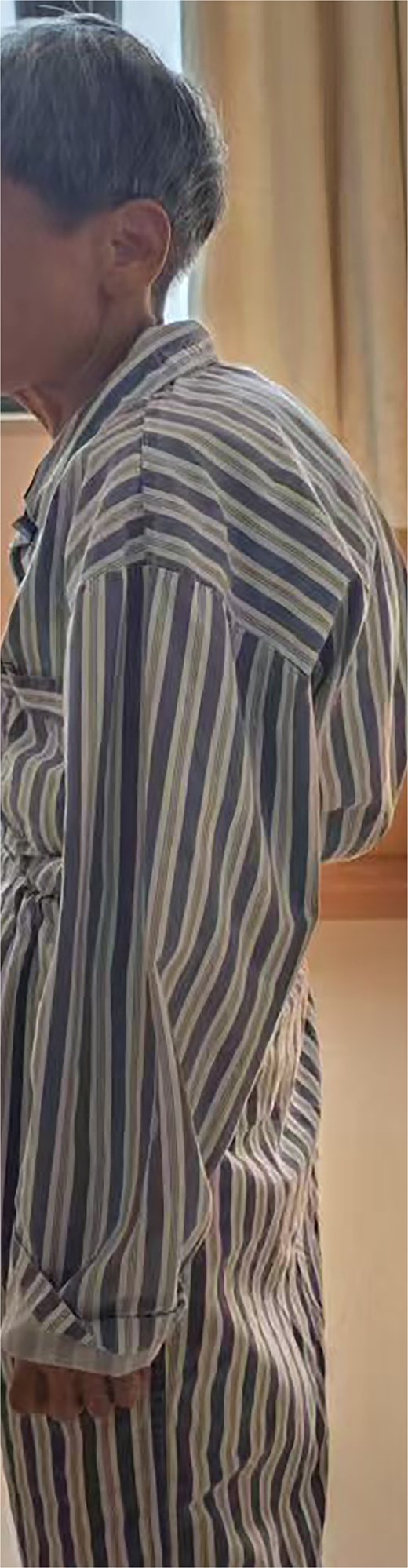
Physical characteristics of the patient.

CT showing a distended gallbladder.
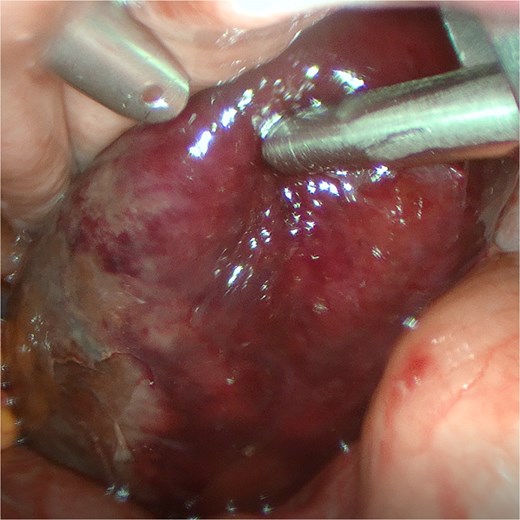
The gangrenous gallbladder founding during the operation.
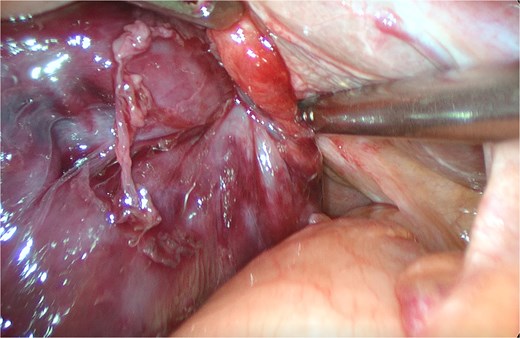
Identification of the twisted part of the gallbladder.
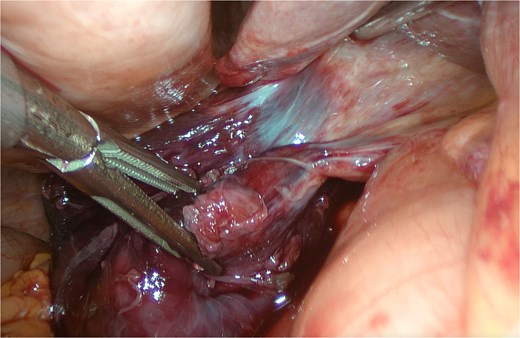
View of the gallbladder after detorsion.
Discussion
Gallbladder torsion is a rare surgical emergency that has been reported across different age groups. The etiology of gallbladder torsion is currently believed to be associated with congenital anomalies such as an elongated gallbladder, as well as non-congenital anatomical factors including perivisceral fat atrophy and increased gallbladder elasticity [5–9]. Although gallbladder torsion lacks specific clinical presentations, Lau et al. [10] reported and summarized three related triads. The patient described in this paper exhibited several distinctive characteristics, including a thin, elderly patient with a deformed spine, typical abdominal pain, a short history, and early onset of vomiting. Based on these clinical features, we argue that elderly patients presenting with similar symptoms should be carefully evaluated due to the possibility of gallbladder torsion. Similarly, there is currently a lack of specific preoperative imaging characteristics for gallbladder torsion. Some reports have suggested that CT findings such as the ‘beak sign’ and ‘whirl sign’ can indicate rotation of the gallbladder pedicle [11, 12]. Reviews have also mentioned that some literature suggests that US examination shows the gallbladder located outside the gallbladder fossa and below the liver, connected to the liver by a conical structure, which corresponds to the twisted gallbladder pedicle [13]. Once gallbladder torsion is definitely diagnosed, emergency cholecystectomy should be performed as soon as possible to prevent progression of the condition to gallbladder necrosis, perforation, and hemodynamic instability. Although the preoperative diagnosis in this case was not correct, timely laparoscopic surgery was performed, and no adverse consequences occurred. A comprehensive understanding of gallbladder diseases extends beyond their typical clinical presentations. Clinicians must conduct a holistic evaluation of the patient—including comorbidities, functional status, and imaging findings—with particular attention to subtle or atypical radiological features. In cases where symptoms persist despite appropriate conservative management and fail to align with established diagnostic patterns, gallbladder torsion should be actively considered as a rare but potentially life-threatening differential diagnosis. Timely recognition and prompt surgical intervention are critical to mitigating morbidity.
Conclusion
By sharing this case, we acknowledge that while the imaging diagnosis of gallbladder torsion remains challenging, we believe that in the presence of a hunched and thin patient with cholecystitis that does not respond to conservative treatment, it is necessary to be vigilant for gallbladder torsion.
Acknowledgements
The authors would like to thank the patient for giving her consent.
Conflicts of interest
There is no potential conflict between all of the authors.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}