





Abstract
Appendiceal neoplasms (AN) are an uncommon condition that are typically diagnosed incidentally following an appendicectomy for appendicitis. However, there has been an increased incidence of AN, thought to be secondary to the increased use of computer tomography scans. Therefore, understanding of a broad range of differentials and management of potential AN is necessary for general surgeons.
This case report describes an exceptionally rare occurrence of three distinct neoplastic processes—mixed neuroendocrine tumor, goblet cell adenocarcinoma, and low-grade appendiceal mucinous neoplasm—coexisting within a single appendix. We believe this case provides valuable clinical and pathological insights into the broad range of AN, highlighting the diagnostic challenges and the role of the multidisciplinary team.
Introduction
Appendiceal neoplasms (AN) are found in 0.9%–1.4% of appendicectomy specimens, most frequently incidental following appendicectomy for appendicitis [1]. Recognized primary AN in the WHO 2025 classification of tumors include low and high grade appendiceal mucinous neoplasms (LAMN and HAMN, respectively), colonic-type adenocarcinoma, signet ring adenocarcinoma, goblet cell adenocarcinoma, neuroendocrine tumors (previously known as carcinoid tumors) and neuroendocrine carcinomas. The concept of collision tumors such as mixed neuroendocrine non-neuroendocrine tumor (MiNEN) has also been described [2], and included in the 5th edition of WHO classification as a distinct entity. In this case report, we describe the extremely rare case of a patient who was found to have three distinct tumor morphologies in her appendix.
Case report
A 49-year-old woman was found to have an incidental 48 × 26 × 19 mm appendiceal mucocoele of the distal appendix on computer tomography (CT) scan of the abdomen and pelvis (Fig. 1). This was on a background of several month history of low grade right lower quadrant discomfort. The CT scan was conducted for assessment of unrelated left sided abdominal pain which was attributed to epiploic appendagitis. Her medical background included supraventricular tachycardia, partial thyroidectomy, hypertension, dyslipidaemia and previous hysterectomy for fibroids.
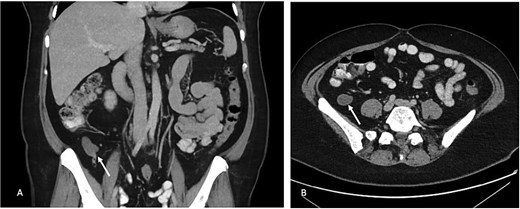
(A) Portal venous phase coronal slice of CT image with arrow pointing to dilated tip of the appendix. (B) Axial slice of same.
She underwent a laparoscopic appendicectomy which revealed a dilated mucocele appendix with a healthy base. There was no evidence of disseminated intraperitoneal mucin. The appendix was removed without spillage. Histopathology revealed a 6x4mm lesion in the body of the appendix with an adjacent mucocele (Fig. 2). The mid-appendiceal lesion was within the lamina propria with focal extension into the superficial muscular layer. The majority of the lesion was made up of classical neuroendocrine tumor, staining positive for chromogranin, synaptophysin and CD56 with a Ki67 proliferation index <1%. Closely apposed and intermixed was a distinct region of mucin consistent with goblet cell adenocarcinoma (Fig. 2C).
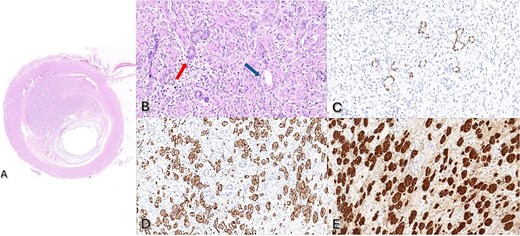
(A) Haematoxylin and eosin (H&E) stain of mid appendiceal lesion with 2x magnification. (B) H&E stain at 40x magnification with red arrow demonstrating goblet cell adenocarcinoma and blue arrow demonstrating neuroendocrine tumor. (C) Positive CDX2 stain consistent with goblet cell adenocarcinoma. (D) Positive CD56 immunohistochemistry and (E) Positive chromogranin immunohistochemistry consistent with neuroendocrine tumor.
The distal mucocele revealed focal villiform mucinous epithelial proliferation with low grade cytological atypia consistent with a LAMN (Fig. 3). In addition, a sessile serrated polyp without dysplasia was present at the base of the appendix, involving the resection margin.
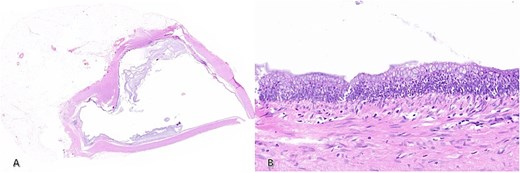
H&E staining of (A) distal appendix at 2x magnification demonstrating the dilated lumen and (B) 20x magnification slice showing dysplasia of the epithelium consistent with LAMN.
The case was discussed at Liverpool hospital colorectal multidisciplinary meeting, and consensus was pT2 disease based on the neuroendocrine component. She underwent right hemicolectomy 3 months after index appendicectomy, which proceeded without complication. There was no residual disease in the resected colon nor any nodal involvement.
Discussion
The incidence of AN, particularly neuroendocrine tumors, is increasing [3, 4]. While the increased use of CT and developments in histopathological analysis may have improved detection of ANs, detection of ANs tends to be incidental due to vague and non-specific symptoms. More research is required to determine genetic and environmental risk factors.
The management of AN varies greatly by type of neoplasm and therefore, it is important that clinicians involved in the care of ANs to maintain an up-to-date understanding of the diagnostic and treatment modalities for AN. In a situation where AN is suspected, a simple appendicectomy is reasonable if the base of the appendix is not macroscopically involved. This case is challenging due to multiple diagnoses present, though it is the presence of goblet cell adenocarcinoma that prompted the decision to proceed to completion right hemicolectomy. Completion right hemicolectomy is generally not recommended for neuroendocrine tumors <1cm [5], but is almost routinely completed for goblet cell tumors [6] though there is a lack of high-level evidence to support this practice. LAMNs confined to the appendix and without disruption intraoperatively are also considered cured with appendicectomy alone.
This case highlights the importance of awareness among clinicians to consider differential diagnoses in appendicitis and establish clear surgical guidelines for intervention. Furthermore, this case displays the importance of multidisciplinary discussions in AN management, especially when there are multiple pathological processes occurring concurrently. We believe, publishing case reports such as ours, enable clinicians, pathologists, radiologists, and oncologists to make more informed decisions and is essential for advancing our understanding of these rare tumors, improving diagnostic accuracy, optimization of treatment strategies, and enhancing patient outcome.
Acknowledgements
The authors would like to acknowledge the contribution of the department of anatomical pathology, colorectal surgery and the multidisciplinary team at Liverpool Hospital for their contributions to this research.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}