





Abstract
Pyogenic liver abscesses (PLAs) are rare, Klebsiella pneumoniae, and Escherichia coli are the most common pathogen of liver abscess. Clinical presentation of PLAs is non-specific, the most common presentation includes fever and rigors, nausea and vomiting, right upper quadrant pain, anorexia, weight loss, weakness and malaise. Untreated, (PLA) is uniformly fatal due to ensuing complications. The peritoneal cavity is the most common location of ruptured liver abscess, a serious surgical emergency. Systemic antimicrobial therapy remains the mainstay primary treatment. We present a rare case of 61 years man with 4 days of intestinal occlusion secondary to a giant pyogenic hepatic abscess that ruptured into the abdominal cavity causing intestinal obstruction resolved by laparoscopic surgery.
Introduction
Pyogenic liver abscesses (PLAs) are associated with uncommon suppurating infections of the hepatic parenchyma. However, their incidence rate is region-dependent. In the United States, bacterial causes account for >80% of all liver abscesses, with an incidence of 4.1 per 100 000 people. Southeast Asia has a high incidence of PLAs [1].
Klebsiella pneumoniae and Escherichia coli are the most common pathogens that cause liver abscesses. Staphylococcus spp. are also associated with trauma-induced liver abscesses. The mortality rate of PLAs is as high as 15% to 20% [2].
Untreated, PLAs are uniformly fatal due to ensuing complications such as sepsis or peritonitis, secondary to rupture of the abscess cavity into the pleural or peritoneal cavities. The peritoneal cavity is the most common location of ruptured liver abscesses, which are serious surgical emergencies. Despite the use of antibiotics in almost all patients with PLA, most require additional interventions [3, 4].
Case report
We present the case of a 61-year-old male, with a medical history of chronic alcohol consumption since the age of 13 years and recreational use of marijuana and cocaine. He presented to the emergency department with a three-month history of involuntary weight loss (30 kg), fatigue, weakness, and diffuse colicky abdominal pain. He presented to the emergency department because of four days of being unable to evacuate, with abdominal distension, and diffuse abdominal pain that had worsened in the previous 24 hours. Abdominal examination revealed severe diffuse abdominal pain, rebound tenderness, and decreased bowel sounds.
Contrast-enhanced computed tomography (CT) of the abdomen revealed a large hepatic abscess 190 × 103 mm, involving segments IVa, V, VII, and VIII, associated with dilated intestinal loops, and perihepatic fluid (Fig. 1).
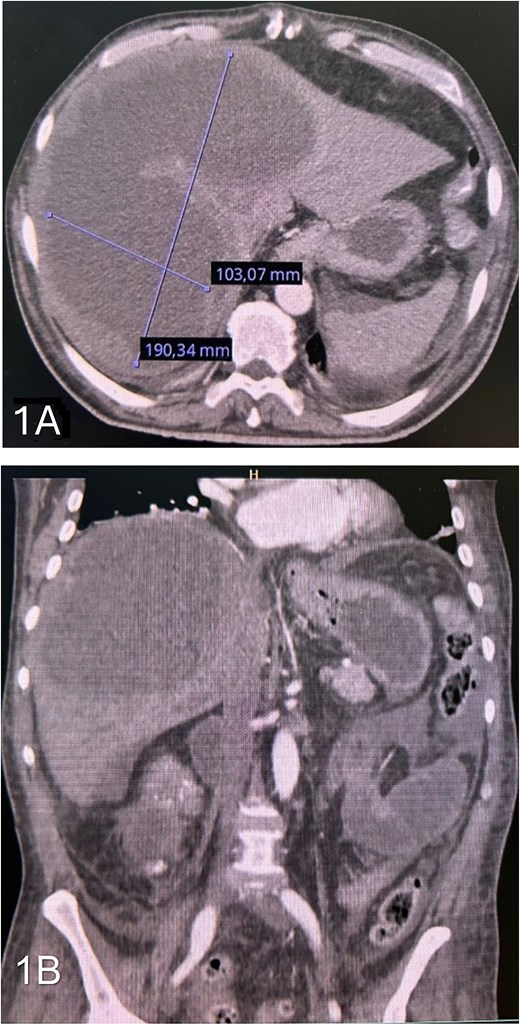
(A) axial contrast-enhanced CT scan showing a large hepatic abscess involving segments IVa, V, VII, and VIII. (B) Coronal contrast-enhanced CT showing free fluid around the bowel and in the peritoneal cavity.
The patient was diagnosed with acute abdomen and intestinal obstruction, and he was transferred to the operation room. Intra-operative findings included a large purulent collection with multiple adhesions to the small bowel, an hepatic abscess in segment VIII containing approximately 300 mL of purulent fluid, and a second abscess in segment V with 200 mL of thick purulent material (Figs 2 and 3).
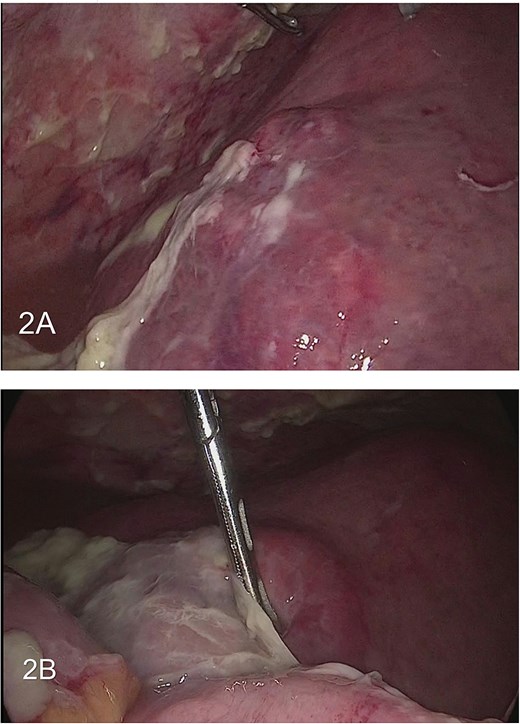
(A) large hepatic abscess with large purulent collection. (B) Purulent collection within the bowel.
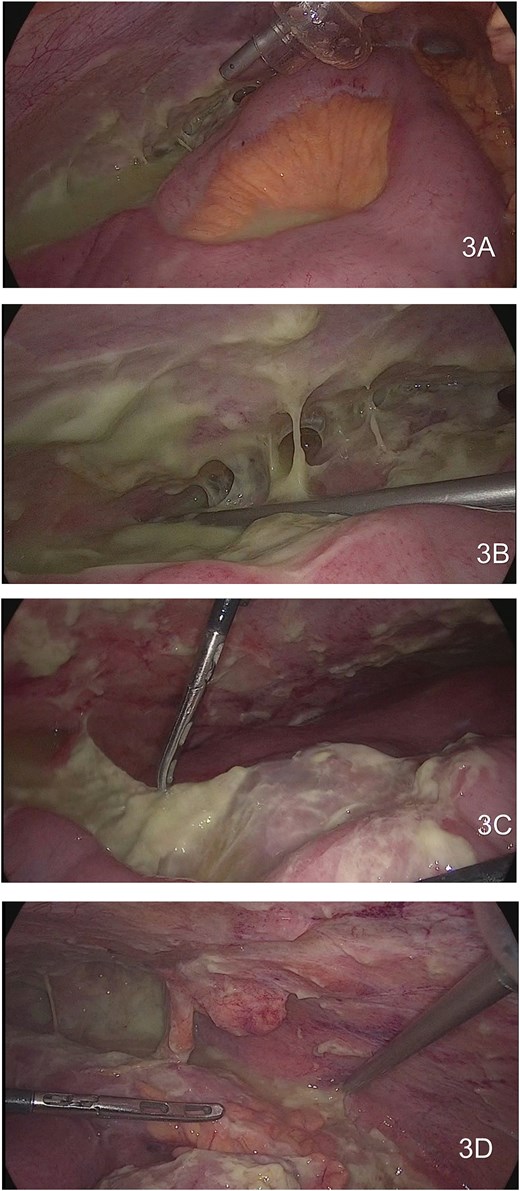
Showing large purulent content that involve the majority of the abdominal cavity. (3A) Right parietocolic gutter and abscess between the intestines. (3B) Right hypochondrium with purulent adhesions. (3C) Multiple fibro adhesion bands in the small bowel. (3D) Purulent content involving in the pelvic cavity.
The large hepatic abscess was evacuated and aspirated. The gallbladder was distended, with adhesions; therefore, a standard cholecystectomy was performed, without complications. The abdominal cavity was cleaned and irrigated with normal saline. A drain was placed inside the abscess cavity (Fig. 4).
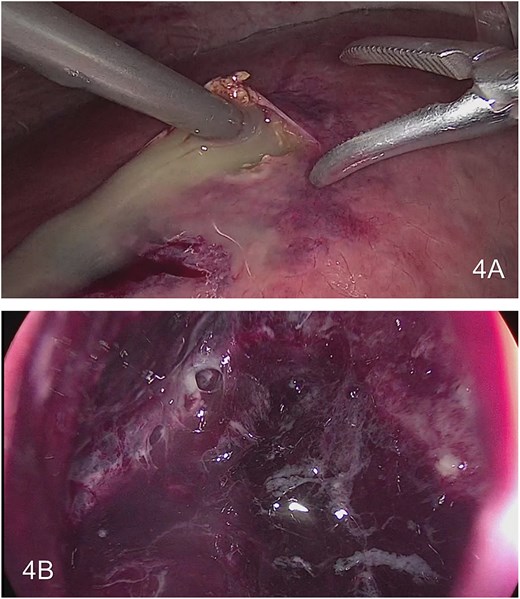
Drainage of large hepatic abscess. (A) Drainage of multiple collection in the liver. (B) View inside the large hepatic abscess.
Cultures of the hepatic abscess revealed Streptococcus constellatus and Fusobacterium spp.
Post-operatively, the patient tolerated oral intake and was discharged without complications, after a 7-day course of intravenous antibiotics. At home, he continued a double oral antibiotic regimen for another 7 days.
After one month, the patient remained asymptomatic. Follow-up CT revealed a marked decrease in intra-hepatic collections (Fig. 5).

Non-contrast abdominal CT scan at 1-month postoperatively showing significant reduction in intrahepatic collection.
Discussion
Hepatic abscess was first described in the time of Hippocrates (approximately 400 BC). In 1938, Ochsner’s seminal review of 47 cases of PLAs heralded open surgical drainage as the definitive therapy [5].
PLAs have an incidence rate of 1.07 to 3.59 per 100 000 people in the West and up to 17.59 per 100 000 people in the East. The etiologies of PLAs have shifted from intra-abdominal infections, such as acute appendicitis and trauma, to pathological conditions of the biliary tract; however, up to 55% of patients with a PLA have no clear risk factors. Uncontrolled diabetes and colorectal cancer are risk factors for the development of cryptogenic abscesses [6].
Liver abscesses can be solitary or multiple. They are more frequent in the right than in the left or both liver lobes. Most abscesses are polymicrobial, with E. coli, Klebsiella, Enterococcus, Bacteroides, and Staphylococcus being the most commonly implicated bacteria. E. coli is mostly responsible in Western countries, whereas K. pneumonia is mostly responsible in Asian countries [7, 8].
The clinical signs of PLAs are often non-specific symptoms that indicate abdominal infection. The most common presenting complaints are fever (90%), abdominal pain (50%–75%), and chills (69%). Less common complaints include nausea, vomiting, weight loss, anorexia or recent unexplained weight loss, headaches, myalgia, and diarrhea. Physical examination can reveal fever, tachycardia, and hypotension. Jaundice is a late symptom of a liver abscess unless there is purulent cholangitis. Due to non-specific symptoms, the diagnosis can be delayed by 4–5 days [1, 3, 4].
Rupture of a PLA is much less common, but it can increase morbidity and mortality. In a retrospective study from Korea of 602 patients with PLA, 23 (3.8%) presented with spontaneous rupture of liver abscess (SRLA). The higher incidence was correlated with Klebsiella-associated PLA, while spontaneous rupture in these patients was significantly correlated with larger abscess size (>8 cm), diabetes mellitus, gas formation, and involvement of the left hepatic lobe [9].
In a comprehensive tertiary care center study on ruptured liver abscesses of 115 patients with SRLA, diagnosed by ultrasound, there was right lobe involvement in 76%, left lobe involvement in 9.5%, and involvement of both lobes in 10%. The most common site of collection rupture was subcapsular (39.1%). This study also reported that 13.9% presented with bowel perforation and the most common site of perforation was the cecum. The mortality rate was 20% [10].
Imaging is the preferred modality for diagnosing liver abscesses. Ultrasonography has a sensitivity of 85%, although contrast-enhanced CT has a higher sensitivity of 95% to 97%. A common liver abscess is a well-defined round lesion with central hypoattenuation, enhancement of the rim and internal septa due to increased vascularity. In the pre-suppurative phase, an abscess can simulate a tumor, appearing heterogeneous with poorly marginated borders and irregular contours. Subsequently, during the suppurative phase, the lesion is hypodense with a thick capsule [11].
Systemic antimicrobial therapy remains the mainstay of primary treatment. The most used empirical antimicrobial regimen is 3rd generation cephalosporin and metronidazole. The recommended duration of parenteral antibiotic therapy is 2–3 weeks. Complementary oral antimicrobial therapy must then be continued for a further 2–4 weeks [7, 12].
Antibiotic therapy alone is usually insufficient to entirely resolve a liver abscess unless it is small (<3 cm). In addition to abscess size, other criteria for percutaneous drainage include continued pyrexia after 48–72 hours of adequate medical treatment and clinical or ultrasonographic features that suggest impending perforation [13].
Indications for surgical intervention include no clinical response after 4–7 days of drainage via a catheter placed in the abscess cavity, multiple, large, or loculated abscesses, a thick-walled abscess with viscous pus, and concurrent intra-abdominal surgical pathology [1, 7].
In a meta-analysis of 17 studies that included patients with liver abscesses, 299 patients were treated laparoscopically. Laparoscopy is an effective alternative to open surgery, by allowing evacuation of the pus. The caudate lobe is an infrequent location but it is associated with a greater risk of rupture. This specific location is more difficult to access by external drainage [14].
Conclusion
PLAs are associated with an uncommon suppurating infection of the hepatic parenchyma that is potentially life-threatening. Rupture of a hepatic abscess is a rare complication, but it is a serious condition that requires surgical intervention. The laparoscopic approach is safe and allows evaluation of the entire abdominal cavity.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}