





Abstract
Olfactory groove schwannomas are exceptionally rare intracranial tumors that present a significant diagnostic challenge, as they are frequently misidentified as meningiomas on preoperative imaging. We report the case of a 44-year-old woman who presented with a two-month history of headache and blurred vision. Neuroimaging revealed a large, dural-based, homogeneously enhancing extra-axial mass in the left frontal region, strongly suggestive of a meningioma. The patient underwent surgical excision of the lesion. Histopathological examination, however, revealed the classic features of a benign schwannoma, including Antoni A and B areas, nuclear palisading, and Verocay bodies. This diagnosis was confirmed by an immunohistochemical profile that was positive for S100 and negative for Epithelial Membrane Antigen. This case underscores the limitations of radiological diagnosis for skull base lesions and highlights the critical role of histopathological and immunohistochemical analysis in achieving a definitive diagnosis, which is paramount for guiding appropriate management.
Introduction
Schwannomas are benign, slow-growing tumors arising from peripheral nerve sheath Schwann cells. While common in the head and neck, particularly the vestibular nerve, intracranial olfactory nerve schwannomas are notably rare [1]. Their non-specific presentation—headaches, visual disturbances, and elevated intracranial pressure—overlaps with other skull base pathologies [2]. The olfactory groove is predominantly associated with meningiomas, extra-axial tumors from arachnoid cap cells. Radiologically, both can appear as well-defined, dural-based, enhancing masses on computed tomography (CT) and magnetic resonance imaging (MRI), increasing pre-operative suspicion for meningioma [3]. This mimicry complicates diagnosis, as surgical planning for excision requires accurate pathological identification.
We present a 44-year-old female with an olfactory groove mass, radiologically classified as a meningioma but histopathologically confirmed as a benign schwannoma. This underscores radiological limitations and histopathology’s essential role in definitive skull base tumor diagnosis.
Case presentation
A 44-year-old right-handed woman presented with a two-month history of headache and blurred vision. Her medical history included hypertension and type 1 diabetes mellitus. She reported gradually worsening intermittent headache and bilateral visual blurring, more pronounced in the right eye. Symptoms exacerbated with physical exertion and were unrelieved by analgesics, leading to her referral. Examination revealed a conscious, alert patient with right eye proptosis. Visual acuity was 6/6 (left eye) and 6/9 (right eye). Fundoscopy identified bilateral Grade 3 papilledema. Non-contrast brain CT demonstrated a well-defined, isodense, dural-based extra-axial lesion in the left frontal region with a cystic component, measuring approximately 5.5 × 4.3 × 4.2 cm. It was associated with mild perilesional edema, mass effect, and a subtle contralateral falx shift. The initial impression was an atypical meningioma (Fig. 1). Subsequent MRI confirmed a large, falcine-based lesion that appeared isointense on T1- (Fig. 2) and T2-weighted images, demonstrating intense homogeneous enhancement post-contrast (Fig. 3). Signal voids suggested calcifications. The patient underwent gross total excision via a bilateral frontal craniotomy. The tumor was intradural and extra-axial, elevating the frontal lobe and was easily accessible; therefore, neither neuronavigation nor other intra-operative localization aids were utilized. Intraoperatively, the olfactory tract could not be clearly identified. A gap in the anterior cranial base was noted, but as there was no evidence of dural invasion or cerebrospinal fluid leak, no sealant was required. Gross examination of the resected specimen revealed a well-circumscribed, white nodule. Microscopically, sections showed benign spindle cell proliferation with alternating Antoni A and Antoni B areas (Fig. 4). Antoni A regions displayed nuclear palisading and Verocay bodies (Fig. 5), while Antoni B areas were edematous and myxoid (Fig. 6). No mitotic figures or atypia were seen. The definitive diagnosis was a benign olfactory groove schwannoma, notable given the initial radiological suspicion of meningioma. Her postoperative course was uneventful. A postoperative non-contrast CT brain obtained 48 hours after surgery confirmed gross total resection (Fig. 7). She was discharged with scheduled follow-up to monitor recovery and visual symptoms.
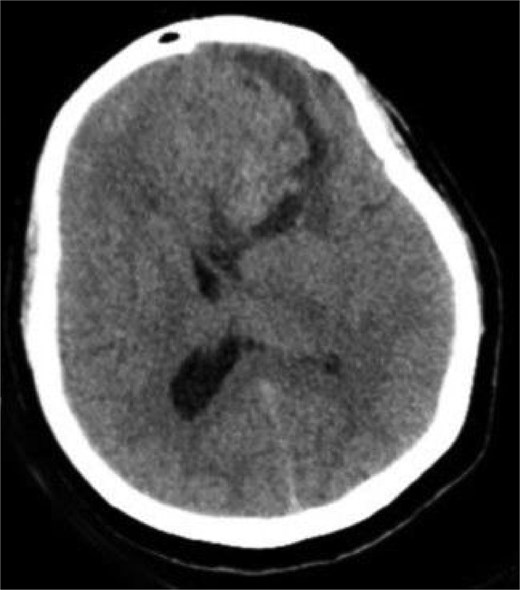
Preoperative CT brain without contrast (axial view) showing a well-circumscribed mass in the right frontal lobe resting on the falx cerebri, causing leftward midline shift with associated vasogenic edema and mass effect.

MRI brain without IV contrast (T1 sequence) showing a well-circumscribed hypointense mass with areas of heterogeneity occupying the right frontal lobe, closely related to the midline structures and falx cerebri.
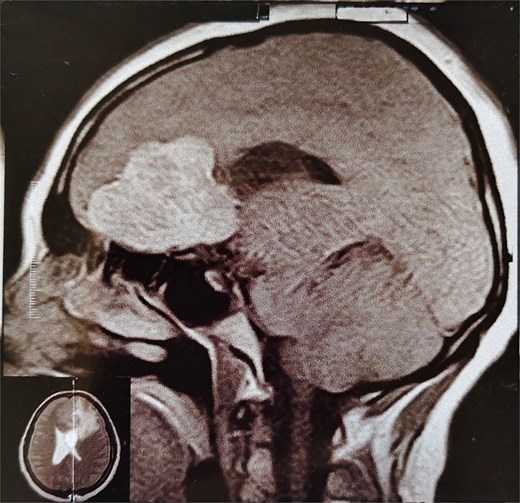
MRI brain with IV contrast (sagittal midline view) showing a homogeneously enhancing mass based on the cribriform plate of the ethmoid, displacing the frontal lobe upward and posteriorly.
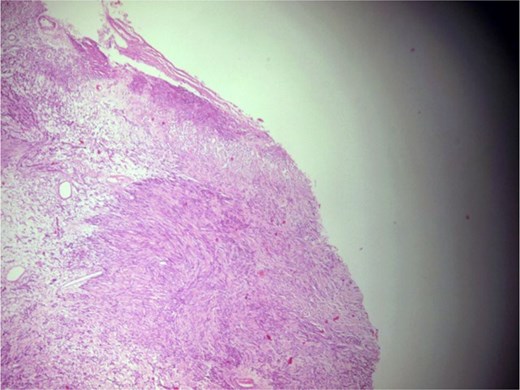
Photomicrograph showing a well-circumscribed, partially encapsulated lesion composed of hypercellular Antoni a areas admixed with myxoid hypocellular Antoni B areas (H&E, ×100).
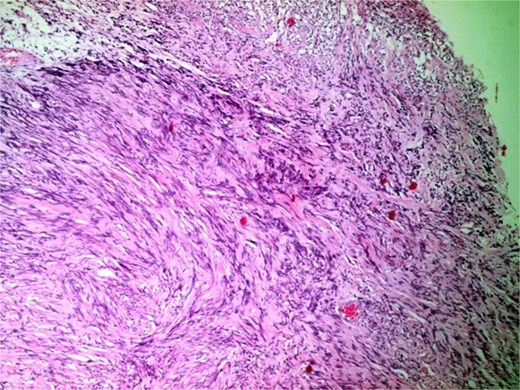
Photomicrograph of hypercellular Antoni a areas showing interlacing bundles of spindle-shaped cells with nuclear palisading (H&E, ×400).
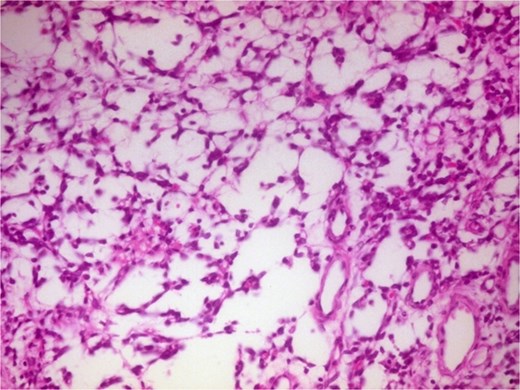
Photomicrograph of hypocellular Antoni B areas showing few cuboidal cells separated by myxoid stroma (H&E, ×400).
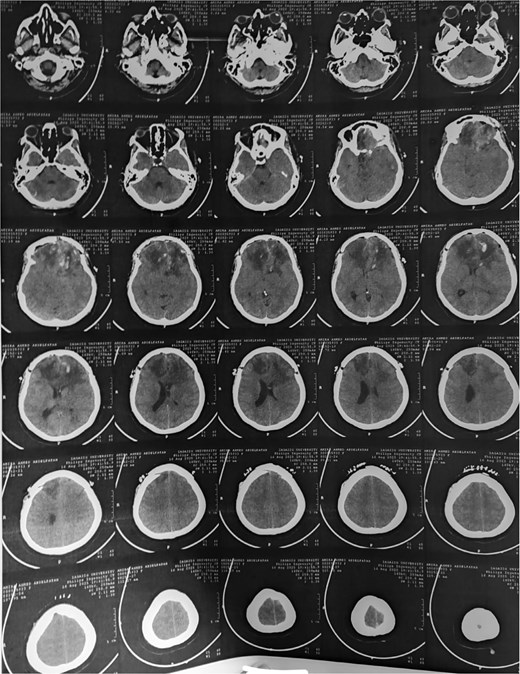
Post-op CT brain showing total excision of the tumor leaving mild post-op oedema at tumor bed.
Discussion
Olfactory groove schwannomas (OGS) are rare and diagnostically challenging, as the olfactory nerve contains few Schwann cells, the typical origin of schwannomas. A 44-year-old woman had a large left frontal extra-axial lesion, initially diagnosed radiologically as a meningioma but later confirmed histopathologically as a benign schwannoma, illustrating this diagnostic dilemma and aligning with literature trends [4–7].
The initial radiological diagnosis of meningioma was understandable. The lesion demonstrated features of an atypical meningioma on CT and MRI: a well-defined, dural-based, extra-axial mass with significant homogeneous contrast enhancement, edema, and mass effect [8]. This diagnostic error is common; most OGS cases are misdiagnosed preoperatively as olfactory groove meningiomas [4–7, 9–12]. Shared radiological features include a dural base, isointensity on T1/T2 sequences, and homogeneous enhancement [4, 8, 9]. However, certain subtle indicators can suggest schwannoma. Cystic components, as in our case and others [4, 8], and the absence of hyperostosis or a prominent dural tail [10, 11], favor OGS. Bone erosion, noted by Shenoy et al. [12] and Murakami et al. [13], is also more indicative of slow-growing schwannomas.
Definitive diagnosis relies on histopathology and immunohistochemistry. Microscopy revealed the classic biphasic pattern of benign schwannoma with Antoni A and B areas, nuclear palisading, and Verocay bodies, a pattern foundational to diagnosis [4–7, 9, 10]. Immunohistochemistry is crucial for differentiation. The tumor cells showed strong, diffuse S-100 protein positivity [4–7, 9] and were negative for Epithelial Membrane Antigen (EMA), which is typically positive in meningiomas [5–7, 9]. This S100-positive/EMA-negative profile is definitive for schwannoma. Additional markers like SOX-10 [4] or CD57 [5, 9] can further distinguish OGS from other rare tumors.
The patient presented with a two-month history of headaches, blurred vision, and papilledema. While anosmia is considered a key symptom, our review found diverse presentations (Table 1). Many patients have olfactory dysfunction [14–16], but a significant number, including ours and others [10, 17], have preserved smell. This suggests symptoms often arise from mass effect on adjacent structures like the optic apparatus and frontal lobes, causing visual issues, headaches, and seizures, rather than direct olfactory nerve involvement [7, 10, 18]. Table 2 summarizes key features from the literature.
Patient demographics, clinical presentation, and olfactory outcomes.
| Study ID | Age | Sex | Main symptom | Pre-op olfaction | Post-op olfaction | Follow-up (Recurrence) |
|---|---|---|---|---|---|---|
| Sousa 2025 | 16 | M | Headaches, hyposmia, convulsion | Hyposmia | Restored | 2 years (No) |
| Vp 2022 | 32 | M | Progressive headaches | Anosmia absent | Asymptomatic | 2 years (No) |
| Masuda 2020 | 13 | F | Headache | Normal | NA | 5 years (No) |
| Taha 2018 | 56 | M | Incidental (RTA), anosmia | Anosmia | No improvement | NA (No) |
| Liby 2016 | 13 | F | Seizures, papilloedema, vision impairment | Diminished sense | Residual anosmia | 6 months (No) |
| Manto 2016 | 39 | F | Headache, loss of smell | Anosmia (right) | NA | 4 months (No) |
| Bohoun 2016–1 | 26 | M | Incidental finding | Anosmia (right) | Unchanged | NA (No) |
| Bohoun 2016–2 | 24 | F | Syncope | Anosmia (right) | Unchanged | NA (No) |
| Quick 2015–1 | 64 | F | Headache | Anosmia (left) | NA | NA (No) |
| Quick 2015–2 | 45 | F | Incidental finding, hyposmia | Hyposmia | NA | NA (No) |
| Kim 2015 | 49 | F | Headache, nausea, vomiting | Preserved | Preserved | 19 months (No) |
| Choi 2009 | 39 | F | Anosmia, frontal headache | Anosmia | Improved | NA |
| Mirone 2009 | 38 | M | Headache, vomiting, visual impairment | Slight hyposmia | NA | 18 months (No) |
| Figueiredo 2009 | 49 | M | Headache, loss of smell | Bilateral anosmia | NA | NA |
| Adachi 2007 | 49 | F | Generalized seizures | Normal | NA | 2 years (No) |
| Murakami 2004 | 30 | M | Intermittent headache | Normal | NA | NA (No) |
| Shenoy 2004 | 55 | M | Generalized seizures | Preserved | NA | NA (No) |
| Praharaj 1999 | 45 | M | Headaches, generalized seizures | NA | NA | NA (No) |
| Ulrich 1978 | 19 | M | Epileptic seizures, visual loss | Unilateral anosmia | NA | 3 years (No) |
Surgical, radiological, and histopathological characteristics.
| Study ID | Tumor location | Key imaging features | Surgical approach | Extent of resection | Olfactory nerve intraoperative finding | Final diagnosis (Confirmed by IHC) |
|---|---|---|---|---|---|---|
| Sousa 2025 | Right frontobasal | Cystic & solid; intense enhancement | Transcortical | Complete | NA | Schwannoma |
| Vp 2022 | Right frontobasal | Homogeneous enhancement; peripheral edema (T2) | Minipterional | Radical | Right tract isolated | Olfactory groove schwannoma |
| Masuda 2020 | Anterior skull base | T1 low, T2 high; strong enhancement | Interhemispheric | Gross Total | NA | Olfactory groove schwannoma |
| Taha 2018 | Right frontal (intra-axial) | MRI not performed | Transcortical | Complete | Nerves not identified | Schwannoma |
| Liby 2016 | Midline anterior fossa | Heterogeneous (solid-cystic) | Frontolateral | Total | Right nerve/bulb absent | Olfactory groove schwannoma |
| Manto 2016 | Right anterior fossa | T1 hypointense, T2 hyperintense | Bilateral frontal | Total | Right tract not identifiable; left intact | Typical Schwannoma |
| Bohoun 2016–1 | Right anterior fossa | T1 hypointense, T2 hyperintense | Frontobasal | Total | Continuity with right bulb | Schwannoma-like tumor |
| Bohoun 2016–2 | Right subfrontal | T1 hypointense, T2 hyperintense | Frontal | Gross Total | Arose from right bulb | Schwannoma-like tumor |
| Quick 2015–1 | Frontal base, nasal invasion | Solid mass with cystic areas | Bifrontal | Gross Total | Left nerve destroyed | Schwannoma WHO I |
| Quick 2015–2 | Olfactory groove | Contrast-enhancing | Fronto-lateral | Gross Total | Left nerve destroyed | Schwannoma WHO I |
| Kim 2015 | Left frontal base | T1 hypointense, T2 cystic; variegating enhancement | Subfrontal | Complete | Nerve preserved | Olfactory groove schwannoma |
| Choi 2009 | Ethmoid to right frontal | Inhomogeneous; solid & rim enhancement | Bifrontal, subfrontal | Total | Olfactory bulb involved | Schwannoma |
| Mirone 2009 | Olfactory groove | Cystic mass with edema; strong enhancement | Frontal, subfrontal | Complete | Left bulb/tract not identifiable; right preserved | Typical Schwannoma |
| Figueiredo 2009 | Olfactory groove | T1 isointense, T2 hyperintense | NA | Complete | Both tracts involved | Schwannoma |
| Adachi 2007 | Olfactory groove | T1 low, T2 high; partial enhancement | Left frontal | Total | Nerve stretched thin | Schwannoma |
| Murakami 2004 | Left anterior skull base | Hypovascular (angiography) | Left frontal | Total | Left bulb involved; proximal tract intact | Schwannoma |
| Shenoy 2004 | Midline anterior fossa | T1 hypointense, T2 hyperintense; honeycomb enh. | Frontotemporal | Total | Ipsilateral bulb thinned; contralateral preserved | Schwannoma |
| Praharaj 1999 | Right frontobasal | Uniformly enhancing (CT) | Bifrontal | Total | Bulbs not identified | Hyalinised Schwannoma |
| Ulrich 1978 | Right anterior fossa | NA | Frontal | Total | Right bulb likely destroyed | Schwannoma |
The patient’s uneventful postoperative recovery and planned monitoring align with the generally excellent prognosis of OGS after gross total resection. The literature shows minimal recurrence rates, with no recurrences in reviewed cases despite follow-ups ranging from months to five years [4, 5, 10, 17, 19]. The straightforward surgical access and gross total resection achieved in this case, without the need for complex reconstruction, further support the favorable management outcome for these lesions.
Conclusion
The diagnostic trajectory of this patient highlights the necessity of clinical vigilance in the evaluation of anterior cranial fossa masses. The radiological findings indicated a meningioma; however, the definitive diagnosis of an olfactory groove schwannoma was confirmed through detailed histopathological examination, which revealed classic schwannoma architecture supported by a definitive S100-positive and EMA-negative immunohistochemical profile. This case highlights the significance of olfactory groove schwannomas, which, despite their rarity, must be considered in diagnostics, as precise identification is essential for informing surgical management. This case demonstrates that gross total resection provides an excellent prognosis, with the possibility of definitive cure and long-term disease control.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Funding
We received no funding in any form.
Ethical approval
Ethics clearance was not necessary since the University waives ethics approval for publication of case reports involving no patients’ images, and the case report is not containing any personal information. The ethical approval is obligatory for research that involve human or animal experiments.
Consent of patient
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Guarantor
The corresponding author.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}