





Abstract
Paraduodenal hernia is a rare congenital internal hernia and an uncommon cause of small bowel obstruction (SBO). We report two cases from a single center: a 48-year-old female with a left-sided hernia presenting with SBO and a postoperative pulmonary embolism, and a 24-year-old male with a right-sided hernia complicated by bowel ischemia requiring right hemicolectomy. Both cases were diagnosed preoperatively using abdominal computed tomography and managed surgically with favorable outcomes. Paraduodenal hernias account for <1% of SBO cases and are classified as left-sided (~75%) or right-sided (~25%). Early recognition and prompt surgical intervention are essential, with open surgery often preferred for complicated cases. These cases emphasize the importance of considering paraduodenal hernia in patients with SBO and a virgin abdomen and highlight the role of vigilant postoperative monitoring to prevent morbidity and complications.
Introduction
Paraduodenal hernia is a rare type of internal hernia resulting from congenital anomalies in embryonic midgut rotation and fixation [1, 2]. It is characterized by herniation of small bowel loops through the paraduodenal fossa—a potential space behind the mesentery of the colon [3–5]. Paraduodenal hernias are classified as left-sided (~75% of cases) or right-sided (~25%) [3–5]. Most cases are asymptomatic and incidentally discovered; however, they may present with recurrent abdominal pain or acute small bowel obstruction (SBO) [6]. Reporting these cases provides valuable insights into diagnosis, management, and outcomes.
Case presentations
Case 1: left paraduodenal hernia
A 48-year-old female with hypothyroidism and no prior abdominal surgeries presented with acute, intermittent left upper quadrant pain and vomiting. Family history was notable for paraduodenal hernia. Laboratory investigations were normal.
Imaging
Computed tomography (CT) abdomen revealed a left-sided paraduodenal hernia (Landzert’s fossa) with herniated small bowel loops (Fig. 1). The CT scan demonstrated a classic configuration of a left paraduodenal hernia involving Landzert’s fossa. Axial images showed a tightly packed cluster of jejunal loops located in the left upper quadrant, positioned posterior to the stomach and lateral to the fourth portion of the duodenum. The inferior mesenteric vein (IMV) and left colic artery formed the medial boundary of the hernia neck, which is a key diagnostic feature distinguishing left paraduodenal hernia from other internal hernias. The mesenteric vessels within the cluster appeared crowded and stretched, converging toward the hernia orifice—an indirect sign of mass effect within the sac. No bowel wall thickening or pneumatosis was identified. The normal C-shaped duodenum was displaced slightly medially due to pressure exerted by the herniated jejunal loops.
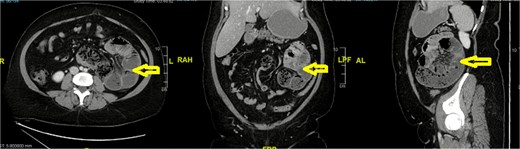
Left paraduodenal hernia (arrow).
Surgical management
During laparotomy, a large left-sided paraduodenal hernia sac was visualized lateral to the fourth part of the duodenum, consistent with herniation into Landzert’s fossa. The IMV formed a prominent band overlying the hernia neck, preventing spontaneous reduction of the jejunal loops (Illustration 1).
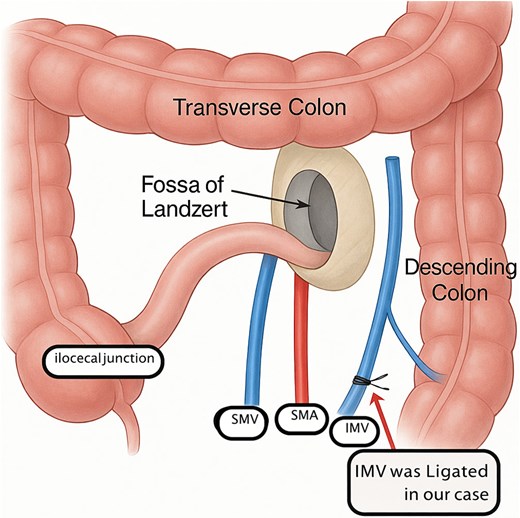
This illustration demonstrates the key anatomical relationships involved in a left paraduodenal hernia. The herniation occurs through Landzert’s fossa, a congenital peritoneal recess located posterior to the IMV and left colic artery, and lateral to the fourth portion of the duodenum. In this diagram, the jejunal loops are shown entering the fossa beneath the IMV, which forms the characteristic vascular boundary of the hernia neck. The transverse colon and descending colon outline the surrounding colonic frame, while the SMA and SMV define the central vascular axis. This configuration reflects the typical mechanism of entrapment seen in left paraduodenal hernias and is important for both radiologic recognition and safe surgical reduction.
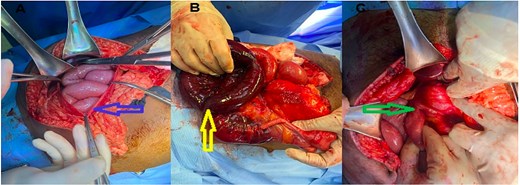
Gentle traction failed to reduce the bowel due to the narrow neck and the overlying IMV. After confirming adequate collateral venous flow, the IMV was safely divided, allowing complete reduction of the herniated jejunum. The bowel was viable throughout. Partial excision of the sac was performed to eliminate the excessive peritoneal pocket and reduce the recurrence risk (Fig. 2).
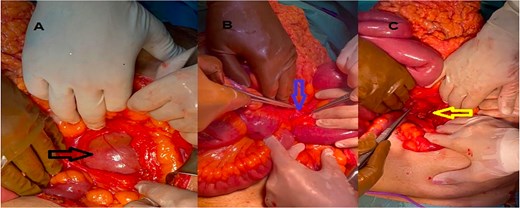
(A) Hernial sac containing bowel (black arrow), (B) IMV (blue arrow), (C) after divison of the IMV (yellow arrow).
Postoperative course
On post operative day 7, the patient developed desaturation and tachycardia. CT pulmonary angiography confirmed pulmonary embolism. She was treated with enoxaparin followed by apixaban for 3 months, with resolution of symptoms.
Case 2: right paraduodenal hernia
A 24-year-old male with no prior medical or surgical history presented with 10 days of diffuse abdominal pain, nausea, and vomiting. Physical exam revealed generalized tenderness. Laboratory tests were unremarkable.
Imaging
CT abdomen showed a large right-sided paraduodenal hernia with malrotation and mildly dilated small bowel loops, with suspicion of ischemia in the terminal ileum and small fluid collection in the pelvic cavity (Fig. 3). CT revealed a right paraduodenal hernia involving Waldeyer’s fossa, characterized by a large cluster of small bowel loops located posterior and lateral to the superior mesenteric artery (SMA). A hallmark feature was the abnormally right-sided duodenojejunal (DJ) junction, indicating an associated rotational anomaly. The SMA formed the anterior margin of the hernia orifice, and the clustered loops were seen passing posterior to this vascular pedicle.
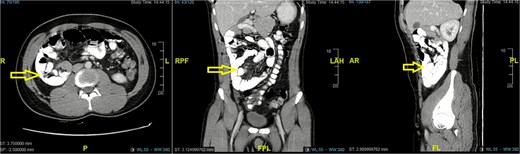
CT abdomen showed right sided paraduodenal hernia (arrow).
Mesenteric vessel crowding and mild swirling were present, raising concern for internal obstruction. The terminal ileum demonstrated focal wall thickening and decreased enhancement, compatible with early ischemia, and there was a small amount of adjacent pelvic free fluid.
Surgical management
Diagnostic laparoscopy revealed significant distention of small bowel loops entering a retro-mesenteric space posterior to the SMA, consistent with herniation into Waldeyer’s fossa. Due to poor visualization and concern for compromised bowel viability, the procedure was converted to open.
Upon opening the hernia sac, ~100 cm of terminal ileum was found to be dusky, congested, and non-viable, confirming ischemia secondary to incarceration. The DJ junction was noted to lie to the right of the midline—an anatomical indicator of associated intestinal malrotation (Fig. 4).
(A) Opened hernial sac with bowel content, (B) ischemic bowel, (C) Duodeno-jejunal junction (DJ) on right side.
A right hemicolectomy with ileocolic anastomosis was performed after resection of the ischemic segment. No further intra-abdominal pathology was present.
Discussion
Paraduodenal hernias are rare congenital internal hernias resulting from abnormal rotation and fixation of the midgut [1–5]. Left-sided hernias herniate through Landzert’s fossa, while right-sided hernias pass through Waldeyer’s fossa. They account for <1% of SBOs and are often diagnosed via CT or magnetic resonance imaging [5, 6].
The pathogenesis of paraduodenal hernia is fundamentally linked to abnormalities in midgut rotation and fixation during embryonic development. Normally, the midgut undergoes a 270° counterclockwise rotation around the SMA during weeks 5–10 of gestation [1, 7]. This rotation occurs in coordinated stages. During the first 90°, the midgut herniates into the umbilical cord, placing the future duodenum to the right and the developing colon to the left. As the midgut returns to the abdominal cavity, it completes an additional 180° of rotation, positioning the duodenum posterior to the SMA and forming the characteristic C-shaped loop. The DJ junction ultimately settles to the left of the midline, anchored by the ligament of Treitz, while the jejunum occupies the left upper quadrant and the ileum descends to the right lower quadrant [1, 3, 5].
Errors during this rotation or in subsequent mesenteric fixation can result in persistent peritoneal recesses that predispose to internal herniation. Such defects give rise to the classic fossae associated with paraduodenal hernia.
Left-sided paraduodenal hernia (Landzert’s fossa)
Left-sided paraduodenal hernias arise from failure of fusion between the descending mesocolon and the posterior parietal peritoneum, resulting in persistence of Landzert’s fossa [3–5]. This recess lies posterior to the IMV and left colic artery, lateral to the fourth part of the duodenum. Herniation typically involves jejunal loops, which become trapped posterior to the IMV—a key diagnostic and operative landmark [3, 4, 7].
Right-sided paraduodenal hernia (Waldeyer’s fossa)
Right paraduodenal hernias occur when the ascending mesocolon fails to properly fix to the posterior abdominal wall, leaving a persistent peritoneal defect termed Waldeyer’s fossa [3, 4, 6]. This space is located posterior and lateral to the SMA. A hallmark feature is an abnormally right-sided DJ junction, indicating an associated malrotation anomaly [2, 6]. Herniated loops often pass behind the SMA, which forms the anterior boundary of the hernia sac and may complicate surgical reduction [3, 6, 7].
Clinical significance
Recognizing these rotational anomalies is essential for diagnosis and operative planning. The IMV in left PDH and the SMA in right PDH are critical vascular landmarks that define the hernial orifice and determine the safety of reducing or enlarging the hernia neck. CT findings, including abnormal DJ position, vessel displacement, and mesenteric crowding, correlate directly with these embryological principles [1, 3–5].
Pathophysiology
The exact pathophysiology of paraduodenal hernia is not fully understood. It is believed to result from a congenital defect in the embryonic rotation and fixation of the mid-gut during development. During embryogenesis, the mid-gut undergoes a 270° counterclockwise rotation around the SMA. Failure of this rotation and fixation can lead to the formation of potential peritoneal recesses, such as the paraduodenal recesses, where herniation can occur [6, 7].
Surgical management
Symptomatic paraduodenal hernias require reduction of herniated bowel and closure of the defect. Open surgery is preferred for complicated cases, such as bowel ischemia or the need for resection, providing superior visualization and tactile feedback compared to laparoscopy [7, 8].
Intraoperative findings
During surgery for paraduodenal hernia, several intraoperative findings may be observed. These findings can vary depending on the extent of herniation and the presence of complications such as bowel obstruction or strangulation. Common intraoperative findings include:
Herniated small-bowel loops: The small intestine is typically found herniating through the paraduodenal recess, either on the left or right side.2
Mesenteric defect: A defect in the mesentery, which allows the bowel loops to herniate into the peritoneal cavity, can be identified.3
Adhesions: Adhesions may be present between the herniated bowel loops and surrounding structures, leading to further complications.
Bowel ischemia: In cases of incarceration or strangulation, signs of bowel ischemia, such as discoloration or necrosis, may be observed.
Reduction of herniated bowel: During surgery, the herniated bowel loops are carefully reduced back into their normal position within the abdominal cavity.1
Closure of defect: The mesenteric or peritoneal defect is closed to prevent future herniation.
Literature review
Selected previously reported cases are summarized in Table 1, highlighting age, side, presentation, management, and outcome.
Selected case reports of paraduodenal hernia
| Author, year | Side | Age | Presentation | Management & outcome | Reference |
|---|---|---|---|---|---|
| Uzunoglu et al., 2016 | Left | 83 | Obstruction; CT: left PDH with intussusception | Laparoscopy → open repair; full recovery | [9] |
| Talreja et al., 2022 | Left | 47 | Recurrent pain; CT: clustered jejunal loops | Laparoscopic repair; uneventful recovery | [10] |
| Kamat et al., 2019 | Right | N/A | Acute obstruction with bowel gangrene | Emergency laparotomy with resection | [11] |
| Sah, 2025 | Left | 59 | SBO; CT: clustered bowel | Laparoscopy → open repair; full recovery | [12] |
| Alabdulaaly et al., 2022 | Right | 21 | CT diagnosis of right PDH | Open repair; uneventful outcome | [13] |
| Al-Darwish et al., 2025 | Right | 38 | Recurrent pain; CT: right PDH | Laparoscopic reduction and defect closure; complete recovery | [14] |
Complications
Pulmonary embolism is a rare but important postoperative complication, as observed in Case 1, emphasizing the need for careful postoperative monitoring and multidisciplinary care.
Conclusion
Paraduodenal hernia, though rare, should be considered in patients presenting with acute or recurrent SBO, particularly in those with a virgin abdomen. Early diagnosis with imaging and timely surgical intervention can prevent severe complications. Open surgical repair remains the gold standard for complicated cases, and vigilant postoperative care is essential.
Author contributions
All authors were responsible for patient care and writing, editing the manuscript.
Conflicts of interest
No conflicts of interest.
Funding
No funding.
Data availability
The datasets used during the current study are available from the corresponding author upon request.
Consent
Written informed consents was obtained from the patients for this study. A copy of the written consents is available for review by the Editor-in-Chief of this journal on request. The information in this case report are completely de-identified.
References
Uzunoglu MY, Altintoprak F, Dikicier E et al. A rare etiology of intestinal obstruction: paraduodenal hernia. J Med Cases 2016;7:223–5.
Talreja DP, Al Aamri HH, Haque PW et al. Paraduodenal hernia: a rare case report. Int Surg J 2022;9:866–9.
Kamat S, Cormoli G, Narsapur S et al. Right paraduodenal hernia, rare cause of gangrene bowel: case report with review of literature. Int Surg J 2019;6:3058–61.
Sah R, Rawal SB, Malla S et al. A left paraduodenal hernia causing bowel obstruction. J Surg Case Rep 2025;2025:rjaf045.
Alabdulaaly N, Alshehri MA, Alsannaa F. Right paraduodenal hernia: a case report and literature review. Int J Innov Res Med Sci 2022;7:173–6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}