





Abstract
Superior mesenteric artery (SMA) pseudoaneurysms are rare but potentially life-threatening complications of chronic pancreatitis. This case report describes a 68-year-old African American female with a history of chronic pancreatitis who presented with acute periumbilical pain. Imaging revealed a 1.2 cm SMA pseudoaneurysm. Given the distal location and high rupture risk, the pseudoaneurysm was surgically resected following laparoscopic localization with open ligation. The patient recovered uneventfully and was discharged on postoperative day 3. This case underscores the importance of early recognition and a multidisciplinary approach in managing SMA pseudoaneurysms.
Introduction
Visceral artery aneurysms (VAAs) and pseudoaneurysms (VAPAs) are rare but potentially life-threatening complications of pancreatitis. These vascular abnormalities are more likely to require surgical intervention in chronic pancreatitis than in acute pancreatitis [1]. A true aneurysm involves dilation of all three arterial wall layers, whereas a pseudoaneurysm results from disruption of the wall, often leaving only the adventitia intact. VAPAs are commonly associated with iatrogenic trauma during vascular or hepatobiliary procedures [2].
Their clinical presentation is often nonspecific, ranging from intraperitoneal or retroperitoneal hemorrhage to gastric outlet obstruction, nausea, vomiting, or diffuse abdominal pain; thus, leading to diagnostic delays and increased risk of rupture and mortality [3]. The splenic artery is involved in ~60% of cases, followed by the hepatic artery; superior mesenteric artery (SMA) involvement is rare, comprising only 6.7% of cases [2].
While many VAPAs are incidentally found on computed tomography (CT) or CT angiography (CTA), SMA pseudoaneurysms are symptomatic in 70%–90% of cases, as in the patient presented here [3]. The main treatment goal is rupture prevention. Endovascular embolization is often preferred due to its minimally invasive nature and faster recovery [4]. Still, open surgery remains the gold standard in cases of failed embolization, anatomical limitations, or hemodynamic instability. Surgical options include aneurysm resection, vessel ligation (with or without reconstruction), or end-organ resection [5]. This case highlights a rare SMA pseudoaneurysm in an African American female with chronic pancreatitis, successfully treated using a modified laparoscopic approach.
Case report
A 68-year-old African American woman with a history of sickle cell trait, Gastroesophageal reflux disease (GERD), hypertension, peptic ulcer disease, asthma, and alcohol use disorder presented with sharp, acute periumbilical abdominal pain for 1 day, accompanied by nausea, vomiting, and non-bloody diarrhea. On examination, she appeared ill and in moderate distress. Her abdomen was minimally distended and diffusely tender, without peritoneal signs.
Laboratory evaluation revealed leukocytosis (12.87 × 109/l), elevated creatinine (1.29 mg/dl), and lipase of 79 U/l. CTA of the abdomen and pelvis showed a 1.2 cm pseudoaneurysm arising from a distal SMA branch and pancreatic calcifications consistent with chronic pancreatitis (Fig. 1).
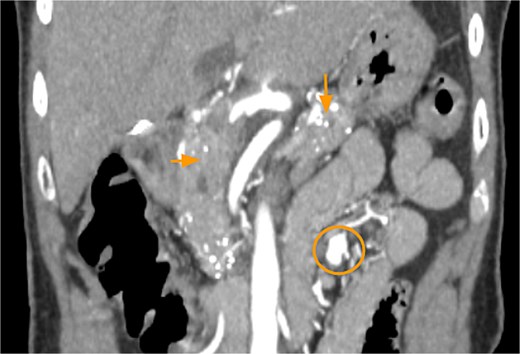
CTA abdomen and pelvis demonstrating pancreatic calcifications (arrows) and SMAP (circle).
Given the pseudoaneurysm’s location in a small, tortuous distal branch, both vascular and acute care surgery teams determined that an endovascular approach was unfeasible. Due to the high risk of rupture and potential bowel ischemia, laparoscopic intervention with possible bowel resection was planned.
The patient underwent diagnostic laparoscopy via a supraumbilical Hasson technique. Intraoperatively, small bowel adhesions were observed in the right lower quadrant and pelvis, but the bowel appeared viable. Upon mobilization toward the ligament of Treitz, a 1.2 cm SMA pseudoaneurysm was visualized proximal to the arcade vessels, with preserved jejunal perfusion.
Due to multiple feeding vessels and its proximity to distal arcade vessels, the procedure was converted to a small laparotomy for definitive control. Feeding arterial branches were suture ligated, and the aneurysmal sac excised (Fig. 2). The mesenteric defect was closed with running 3-0 Vicryl suture. Intraoperative Doppler confirmed preserved small bowel perfusion. The abdomen was irrigated and inspected, and the fascia and skin closed in layers. The patient was extubated and transferred to the post-anesthesia care unit in stable condition.
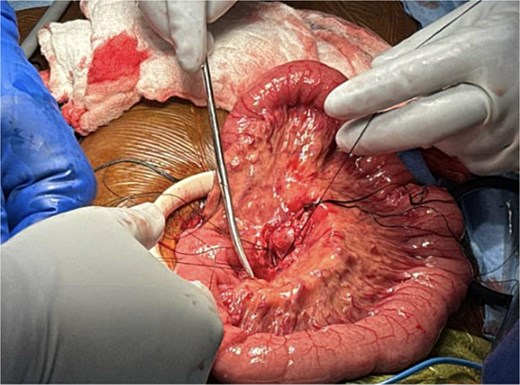
Ligation of feeder vessels to pseudoaneurysm.
Recovery was uneventful. The patient’s pain resolved, bowel function returned, and she tolerated diet advancement. She was discharged home in good condition on postoperative day 3 without complications.
Discussion
SMA pseudoaneurysms are rare but serious vascular complications, especially in the setting of chronic pancreatitis. Although pseudoaneurysms are more common in acute pancreatitis due to sudden enzymatic vessel wall degradation, their formation in chronic pancreatitis is less frequent and often underrecognized.
Chronic inflammation and progressive peripancreatic fibrosis can gradually erode nearby arterial walls through recurrent low-grade enzymatic activity [6]. Perivascular fibrosis may entrap arteries, weaken vessel walls, and lead to delayed pseudoaneurysm development. These vascular lesions may go unnoticed due to overlapping symptoms of chronic pancreatitis.
Endovascular approaches have significantly evolved, now favored in stable patients due to lower morbidity and shorter hospital stays. Embolization materials include coils, cyanoacrylate glue, or gelatin sponge, with success rates over 80% in selected cases [6]. However, some pseudoaneurysms—due to location, size, or patient instability—are not amenable to endovascular therapy, necessitating open surgical management. Surgical options include aneurysm resection, vessel ligation (with or without reconstruction), and, when necessary, bowel resection [7].
Early detection remains a challenge. Routine surveillance imaging is not standardized but may benefit high-risk patients using contrast-enhanced CT or MR angiography [7]. Further research is needed to establish optimal screening intervals, imaging modalities, and cost-effectiveness.
Prevention strategies should focus on modifiable risk factors. For patients with chronic pancreatitis, alcohol and smoking cessation, as well as glycemic control in diabetics, are essential to reducing inflammation and preventing vascular complications. Smoking, in particular, is implicated in the progression of chronic pancreatitis and its vascular sequelae [7].
Management of SMA pseudoaneurysms requires a multidisciplinary team, including gastroenterologists, vascular surgeons, interventional radiologists, and acute care surgeons to ensure timely diagnosis and individualized treatment. Continued research is needed to define best practices for long-term surveillance and evaluate prophylactic strategies for high-risk patients.
Acknowledgements
The authors declare that they have no financial relationships or conflicts of interest relevant to this case report. No institutional or agency support was received for this work.
Conflict of interest statement
The authors declare that they have no financial or personal conflicts of interest relevant to this case report.
Funding
The authors declare that no funding was received for this study.
References
Stanley JC, Wakefield TW. Overview of visceral artery aneurysm and pseudoaneurysm. In UpToDate. 2015, Wolters Kluwer. Retrieved July 11, 2025, from https://www.uptodate.com/contents/overview-ofvisceral-artery-aneurysm-and-pseudoaneurysm

{kind=link}
{kind=link}