





Abstract
A 21-year-old parous woman (G2, P1) presented with sudden abdominal pain in a state of hemodynamic shock. Despite 10 weeks of amenorrhea and a serum β-human chorionic gonadotropin (β-HCG) level >10 000 U/l, several ultrasound (US) scans in another facility failed to detect intrauterine pregnancy. Her history includes past motor vehicle accident. During emergency laparotomy, a moderate amount of hemoperitoneum was seen with a normal uterus and adnexa. A right-sided pelvic wall hematoma was noted. Abdominal US and computed tomography scans demonstrated a large retroperitoneal hematoma with active bleeding. The hematoma spanned from the liver to the pelvic brim with a central cyst-like structure that resembled a gestational sac. During an upper midline laparotomy performed by a multidisciplinary team, the hematoma was evacuated. Histopathological examination of structures within the clot identified chorionic villi. The patient underwent blood transfusions and recovered uneventfully under proper antibiotic prophylaxis. β-HCG levels dropped to zero within 2 weeks.
Introduction
Retroperitoneal ectopic pregnancy (RPEP) is extremely rare, with only 55 cases reported worldwide [1, 2]. Its estimated mortality reaches 5/1000 [3], outnumbering its tubal counterpart by a factor of 10 (0.5/1000) [4, 5]. Late diagnosis can lead to life-threatening hemorrhage since trophoblast invasion causes bleeding or organ rupture [6].
The proposed mechanism for RPEP includes trophoblast migration along lymphatics [7], iatrogenic implantation during in vitro fertilization (IVF), or a retroperitoneal fistulous tract [8]. Risk factors involve endometriosis, myomectomy, intrauterine devices, pelvic inflammatory and sexually transmitted disease.
Case report
A 21-year-old patient was admitted in a state of shock, with abdominal pain of increasing intensity and anemia in the absence of vaginal bleeding. Despite 10 weeks of amenorrhea and positive pregnancy tests, intrauterine pregnancy was not detected on serial ultrasound (US) scans in another facility. In the early morning of 11 July 2024, she experienced sudden, acute abdominal pain, collapsed, and was brought to our hospital by an emergency medical team.
Upon admission, the patient was hypotensive (60/80 mm Hg) and slightly tachycardic (100 bpm). Laboratory tests demonstrated hemoglobin of 104 g/dl, leucocytosis (21.6/μl), and normal platelet count.
Her medical history included injury as a cyclist hit by a car 7 months ago, with fractures of her right fibula, Th12, and L1 vertebrae. Her gynecological history included one vaginal delivery, regular menstrual cycles. β-HCG levels 5- and 2 days prior were 10 000 and 9878 mIU/ml (9 g.w.).
Initial ultrasonography showed a uterus with a decidual reaction of the endometrium without a gestational sac, free fluid in front of the uterus, in the Douglas pouch, and the hepatorenal recess.
A Pfannenstiel laparotomy was performed due to a suspected ruptured tubal pregnancy, revealing 200 ml hemoperitoneum with an intact uterus and adnexa. Unexpectedly, hemorrhagic imbibition of the peritoneum of the right posterior pelvic wall was seen. In the absence of a visible source of bleeding, curettage of the uterine cavity was performed, and the abdomen was closed. Post-surgery hemoglobin dropped from 103 to 76 g/l, for which she received two units of blood and one unit of fresh frozen plasma (FFP).
She underwent abdominal sonography followed by contrast-enhanced computed tomography (CECT). Both demonstrated a right-sided retroperitoneal hematoma adjacent to the inferior vena cava and right kidney. A 5 cm ring-shaped structure resembling an empty gestational sac was detected inside the hematoma (Fig. 1). CT showed contrast extravasation representing active bleeding (Figs 2 and 3). Interdisciplinary team discussion, including obstetrician-gynecologists, abdominal surgeons, anesthesiologists, and radiologists, led to the decision for emergency relaparotomy.

Venous phase coronal plane CECT of the abdomen and pelvis demonstrates a large right-sided retroperitoneal hematoma with a central cystic structure, consistent with a gestational sac. A focus of contrast extravasation is visible medial to the sac. The * symbol denotes blood tracing along the ovarian vessels toward the right pelvic wall, also seen on surgery.
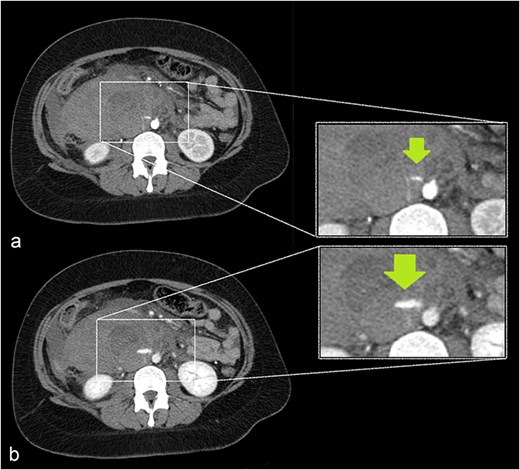
A growing slit-like focus of active extravasation was detected on arterial (a) and venous (b) phase scans, obtained 30 and 70 seconds after contrast injection, respectively.

Sagittal plane CECT shows the hematoma (H) displacing the pancreas ventrally, proving its retroperitoneal location. Active bleeding is seen adjacent to the gestational sac (arrow). A normal appearing, nonpregnant uterus is also visible.
A xyphopubic midline incision revealed a moderate amount of blood in the abdominal cavity, and a large retroperitoneal hematoma, reaching the capsule of both kidneys, bifurcation of the aorta, displacing the head of the pancreas. A total of 1500 ml of blood and clots were evacuated. A membranous structure originating between the vena cava and aorta was removed, leaving a 5 cm bed packed with hemostatic sponges (Figs 4 and 5). Exploration and lavage of the entire abdominal cavity were performed, with drain placement – one retroperitoneal, one right lateral gutter, and one pelvic. During surgery, 606 ml of red blood cells and 350 ml of FFP were transfused. An initial bolus of tranexamic acid (Medocapron) was given during the first laparotomy, followed by an infusion of 1.0 g in 0.9% NaCl under coagulation monitoring at a rate of 80 mg/h from the 8th hour on.
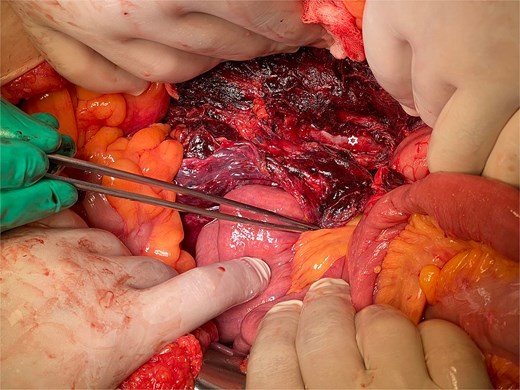
The lesion bed in the retroperitoneal space after hematoma extirpation.

The image displays the membranous structure extracted from the bed, histologically confirmed to represent the gestational sac.
Histopathology on day six confirmed the diagnosis of RPEP, with the presence of blood, fibrin, and chorionic villi (Fig. 6).
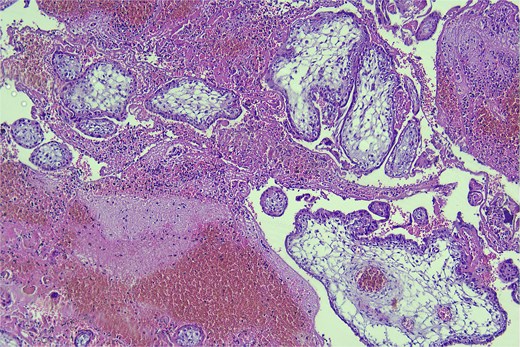
Hematoxylin and eosin stain, high-power magnification (400×) of the surgical material, demonstrating blood, fibrin, and chorionic villi.
The patient was discharged on day eight with decreased β-hCG levels – 272 mIU/ml.
Discussion
RPEP is the type of pregnancy with the lowest incidence and highest maternal mortality. Being in proximity to large vessels, the gestational sac can infiltrate them, resulting in life-threatening bleeding [9].
Several hypotheses for RPEP have been proposed
(i) Lymphatic migration: fertilized oocytes detach and infiltrate compromised lymphatic capillaries, migrating to the retroperitoneal compartment [4, 7].
(ii) Implantation transfer: the embryo initially adheres to the peritoneal surface, subsequently invading the retroperitoneum through trophoblastic invasion [2, 3, 10].
(iii) Fistulous tract formation: following a salpingectomy, the resected end of the fallopian tube may establish a fistulous connection with the retroperitoneum, leading to implantation of the embryo in the peritoneal defect [8].
(iv) Endometriosis: the fertilized ovum may implant on superficial endometriotic lesions, subsequently migrating toward retroperitoneal structures [11].
Our patient had an uneventful vaginal delivery, no abortions, no curettages, or tubal sterility. The patient’s only relevant history was of abdominal trauma during a traffic accident. A study by Cigerci et al found abdominal injuries to be present in as many as 23% of patients with traumatic thoracolumbar fractures [12]. The position of the gestational sac is just below the level of the fractured L1 vertebra (Fig. 7) could suggest an association of RPEP with previous abdominal trauma.

CECT of the abdomen and pelvis in the sagittal plane, bone window. Gestational sac (H for hematoma) was implanted just inferior to the level of a previous traumatic L1 vertebral fracture (arrow).
Findings on US and CT, suggestive of RPEP, are the visualization of an empty uterus with a gestational sac or mass in the retroperitoneal space [13].
Surgical excision of ectopic pregnancies located near major blood vessels parallels lymph node dissection in gynecological malignancies. Consequently, it is recommended that the surgeon performing the excision be a specialist in gynecologic oncology or an expert in retroperitoneal anatomy. Postoperatively, regular monitoring of the patient’s plasma β-hCG levels should be done weekly or every 2 days for patients undergoing conservative management, aiming for two consecutive negative results [14].
Tranexamic acid, an antifibrinolytic agent, was administered intraoperatively to reduce the risk of excessive bleeding and help maintain hemostasis during surgery. Its use should be tailored to the patient’s coagulation status and bleeding risk.
Conclusion
RPEP is an extremely rare and potentially life-threatening condition that requires high clinical suspicion and prompt intervention. The key to successful management lies in early diagnosis and timely surgical intervention to control bleeding and remove the ectopic pregnancy. Close postoperative monitoring and follow-up are essential to ensure full recovery and prevent complications. A coordinated multidisciplinary approach is vital for the best possible outcomes in these complex cases.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}