





Abstract
Colon lipoma is a benign non-epithelial neoplasm. It manifests clinically at an average age of 65 years when it is >2 cm. Treatment depends on its dimensions and complications and consists of endoscopic or surgical resection. One of its complications is intestinal intussusception, which is rare; in adults it represents 5% of all intestinal intussusceptions and only 0.08% of all abdominal surgeries. Here we report the case of a 32-year-old woman with ileocecal intussusception due to a giant submucosal lipoma of the colon, who underwent surgery through a right hemicolectomy with ileostomy, which allowed a favorable outcome for the patient. He has been followed up with no complications identified to date.
Introduction
Submucosal lipoma of the colon (SLC) is a rare benign mesenchymal neoplasm, with a higher incidence in women, typically diagnosed at an average age of 65 years [1]. SLC usually manifests clinically when it exceeds 2 cm in size. Differential diagnoses for SLC include colon polyps and malignant tumors [2]. Treatment is based on the tumor’s size and complications, and typically involves surgical or endoscopic resection [3]. One significant complication of SLC is intestinal intussusception (II), which is most commonly seen in children, but is much rarer in adults, accounting for 5% of adult intussusceptions [4]. The global incidence of II in adults is estimated at 2–3 cases per 1 000 000 people per year. We report the case of a 32-year-old woman with ileocecal intussusception due to a giant submucosal lipoma of the colon, which was resolved by right hemicolectomy with ileostomy, resulting in a favorable outcome [5].
Case presentation
A 32-year-old female patient was admitted to the emergency department with a clinical picture of postprandial abdominal pain predominantly on the right side, persisting for 18 months. Associated symptoms included nausea, constipation, difficulty passing gas, weight loss, and an increase in volume in the right side of the abdomen, worsening over the last 24 h. The abdominal examination revealed distension, asymmetry with increased volume in the right abdomen, and pain on palpation, particularly in the right flank, with a positive rebound sign.
Vital signs on admission were stable: heart rate 82 beats per minute, blood pressure 115/62 mmHg, respiratory rate 19, temperature 36.7°C, and oxygen saturation 96%. A computed tomography scan showed ileocecal intussusception with a ‘donut’ sign, wall thickening of the cecum, and a 16 cm segment of intussuscepted ileum with pneumatosis in the cecum.
Surgical intervention, specifically a right hemicolectomy with ileostomy, was performed. The patient showed improvement and was discharged 5 days after surgery. Two months later, intestinal transit restoration was performed without complications, and she has been followed up with no adverse events to date (Fig. 1).
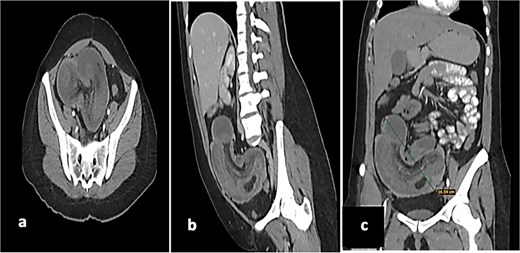
(a) Axial tomography shows the donut sign, thickening of the cecum of up to 10 mm, with reinforcement of the mucosa and muscles, as well as hypodensity of the submucosa. (b) Sagittal tomography showing a loop of ileum and mesentery that are introduced intraluminally into the cecum and ascending colon. (c) Coronal tomography showing a 16 cm long segment of ileum with intussuscepted pneumatosis in the cecum and ascending colon.
An exploratory laparotomy was performed, finding ileo-cecal intussusception with compromise of the ileo-cecal valve and ascending colon, proximal dilation of the small intestine and edema of its wall. Therefore, a right hemicolectomy with ileostomy was performed. The cause of the ileocolic intussusception was an 8 cm submucosal lipoma of the colon (SLC) according to the result of the histological study (Fig. 2). The histological study of the surgical specimen reported an 8.0 cm ulcerated SLC and ileocecal ischemic necrosis secondary to intestinal intussusception of an 18 cm long segment of ileum (Fig. 3).
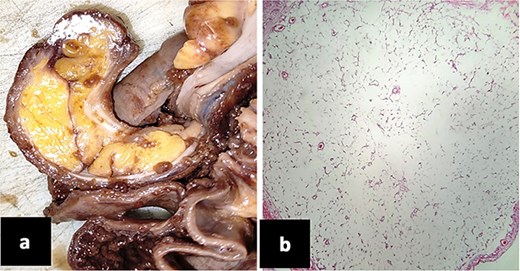
(a) Surgical piece where an 8 cm by 2 cm polypoid lesion is observed in the colon, ulcerated, yellow and fatty in appearance. (b) Microscopic photography. Submucous cecal lipoma made up of numerous mature adipocytes.

Product of hemicolectomy and ileum segment measuring 18.0 × 2.0 cm, tubular and ischemic in appearance with clear loss of usual architecture due to ileocecal intestinal invagination.
Discussion
SLC, first described by Bauer in 1757, is rare and accounts for ⁓0.15% of cases detected during colonoscopy and 0.4%–4.4% of autopsies [6]. It is the third most common benign colon tumor after hyperplastic and adenomatous polyps [7]. The average age at diagnosis is 65 years, with a higher incidence in women. However, giant lipomas can also occur in younger individuals, as evidenced by a case of a 29-year-old patient with a 12.5 cm colonic lipoma causing intussusception [8–11].
The etiology of SLC is not well understood, but it is thought to arise from mesenchymal tissue composed of well-differentiated adipose tissue [12]. These tumors typically originate from the submucosa, though they can extend into the muscularis propria or even subserosa in some cases. Theories suggest that chronic irritation, inflammation, and circulatory deficiencies may contribute to the accumulation of fatty tissue. Genetic abnormalities, including mutations in chromosomes 12q13-15, deletions of 13q, and rearrangements of 6p21-33, have been linked to conditions such as hereditary lipomatosis multiplex, Gardner syndrome, and Cowden syndrome [13].
SLCs are most commonly located on the right side of the colon and are typically solitary, though they can be multiple in up to 10% of cases. In the reported cases of Berna Ayta et al., five were in the ascending colon, one in the hepatic flexure, and one in the splenic flexure, which aligns with the location of the lipoma in our patient [14, 15].
Conclusion
Although the incidence of SLC is low, it is important to consider it within the diagnoses in patients with intestinal obstruction, in which case the treatment is surgical.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}