





Abstract
Manubrio-sternal dislocations (MSDs) are a rare entity that requires high-intensity energy trauma. It can be associated with complex fractures that can be challenging to manage. We aim to present our surgical approach to an MSD associated with multiple chondrosternal joint fractures and underline the mechanism of these rare traumatic chest wall damages. A 39-year-old male suffered from a forklift truck mishap. He arrived at our tertiary center with posterior MSD and chondrosternal joint fracture, lung contusion, pneumothorax, and right humerus fracture. He underwent an open reduction of the sternum and fixation by a sternal plate, bilateral costal osteosynthesis, and humerus fixation. Thoracic cage fracture associated with MSD leads to instability and higher morbi-mortality. Therefore, the surgical approach must be based on the surgeon’s experience and procedures to optimize thoracic cage stability, which must remain the primary objective. We herein report our surgical approach regarding a complex MSD.
Introduction
The manubriosternal joint and the costal rib stabilize the thoracic cavity and protect vital thoracic structures. Due to its strong amphiarthrodial joint covered with hyaline cartilage on both surfaces connected by a fibrocartilage meniscus, manubrio-sternal dislocations (MSD) are rare and occur after high-intensity energy trauma. There are two types of dislocation, whether the sternum body is displaced posteriorly (type I) or anteriorly (type II) from the manubrium. We herein report our surgical approach, management, and outcome of a complex chest wall trauma.
Case report
A 39-year-old male was admitted to our department after a severe crush with a forklift truck on his ribcage/thorax while at work. On arrival, he was conscious with stable vital signs (blood pressure 151/73, heart rate: 78 bpm, and saturation of 100% under 5 l) but complained of heavy right arm and chest pain. The clinical examination revealed an obese patient with a calculated BMI of 41 with a hematoma over the sternum and increased tenderness to palpation with no apparent instability. Deformity of the right arm with nerve damage in the radial territory was also noted. He had no previous medical history. The 3D computed tomography (CT) showed a type I MSD with osteochon dral dehiscence at the level of rib two bilaterally on the sternal side and ribs 4–6 left on the costal side with non-displaced bowing rib fracture of ribs seven and eight anteriorly on the left. An associated small pneumothorax, restricted pneumomediastinum, and the presence of a lung contusion posteriorly on both sides. No laceration, no pleural fluid (Fig. 1). The radiography of the arm showed a transverse, multi-fragmentary mid-diaphysis humeral fracture with bayonet position and significant angulation. The patient was first admitted to the intensive care unit (ICU) for surveillance; pain management was provided with a patient-controlled intravenous analgesia (PCIA) opioid pump, and 3-liter oxygen therapy was administered. The indication for reduction was primarily the severe displacement of the manubrio-sternal junction associated with the chondro-costal dehiscence. The overall stability of the fracture was challenging to assess due to the severe obesity, making a closed reduction even more difficult. Regarding the imagery, we assume that the thoracic cage’s overall stability would be insufficient. Secondly, the patient presented with persistent pain with the need for intravenous opioids. Finally, the patient had to undergo another operation for which the same general anesthesia could stabilize both fractures. After four days of scheduling, the patient underwent a chest wall reconstruction under general anesthesia associated with a patient-controlled epidural analgesia (PCEA). The patient was installed in a supine position with arms abducted. A 15 cm bi-submammary incision up to the sternal fork was realized. Dissection until manubriosternal dislocation was retrieved, reduction was obtained with two 8-hole locking compression plates and secured with 16- and 18-mm screws. Since the chondro-sternal fracture was not eligible between the cartilage and bone for direct osteosynthesis, we performed a fixation at the level of ribs 4–5 bilaterally using titanium rib clip plates stabilized between them by a titanium connecting bar. An open reduction with internal fixation treated the humeral fracture with 4,5 mm 10-hole plates. The patient was extubated directly after the procedure and received postoperative physical and respiratory therapy. He was discharged on postoperative day 4. After two months, the patient still presents limited mobilization on his right hand but has evolved favorably on the thoracic sides with no signs of sternal instability. His radiography showed a correct alignment of the manubriosternal joint (Fig. 2).

Sagittal view on a CT-thorax of the MSD type 1.
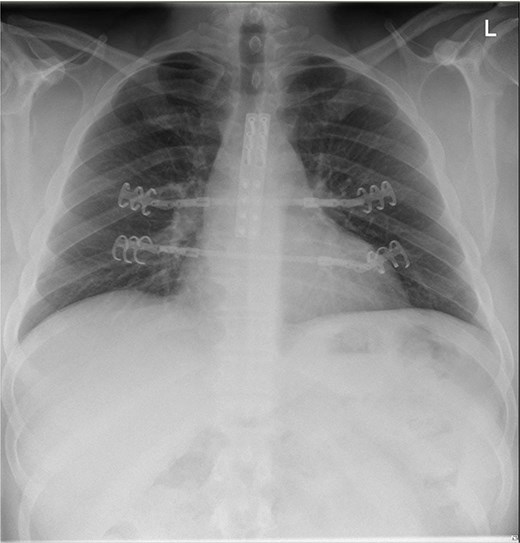
RX thorax of the postoperative reconstruction.
Discussion
The manubriosternal joint is an amphiarthrodial joint, which is reinforced by sternocostal ligaments that provide a strong fibrous mesh conjoining the rib periosteum with the costal cartilage. It is further stabilized by the strong synchondrosis that articulates with the second rib. These strong connections make MSD uncommon, with a prevalence of only 1.3%–3% of all traumatic injuries [1]. The relationship between the sternum and ribs through the sternocostal articulation plays a key role in the stability of the thoracic cage.
Consequently, sternal traumatism is often associated with bilateral rib fractures or flail chest injuries due to direct blunt trauma [2]. The association between both injuries leads to a 40% higher risk of intubation, a 10%–30% higher risk of respiratory failure, and a 10%–40% higher risk of mortality [3].
MSD is frequently noticed in polytrauma patients, where CT scanning is particularly interesting in assessing other injuries such as pulmonary contusion, pneumothorax, or retrosternal hematoma [4].
A review conducted by Fitzpatrick et al. showed the benefits of flail chest fixation in patients regarding the length of ventilation support, ICU stay, rates of pneumonia, mortality, residual chest wall deformity, and total cost of care [5]. However, some cases present complex fracture locations and characteristics where conventional surgical stabilization is challenging to apply.
The management of MSD associated with flail chest is, therefore, challenging. Published literature is often based on small reviews or case reports. Different methods, such as Kirchner wires and plates, have been described with good results [6]. Despite this, plates seem to have better results. In a small case series conducted by Divisi and Crisci comparing the use of surgical steel monofilament vs titanium screws and plates in traumatic sternal dislocations, the latter showed better outcomes regarding shorter hospital stays, lower iatrogenic complications, and fewer chances of reoccurrence [7].
In bilateral rib fractures associated with sternal fractures, a few studies report the uses of a retrosternal metal bar from the well-known Nuss procedure. However, the sternal fracture must also be considered. Other minimally invasive techniques have also been described but remain indicated in properly selected patients [8].
In the present case, MSD was associated with multiple chondro-costal fractures. Our approach was to retrieve the stability of the rib cages and prevent further dislocations. We chose to fix the MSD with plates that, in our opinion, give better stability and less chance of reoccurrence. In our case, adding a titanium connecting bar seems essential to provide steadiness to the rib cage. We are the first to describe this surgical technique. This could be an approach in patients presenting with MSD associated with two or more coastal or chondrosternal fractures. We believe that this approach is safe and reliable. In our cases, the oxygen therapy was stopped the day after the intervention, and the PCEA was removed two days postoperatively. The patient was discharged four days later.
Two months postoperatively, the patients showed no instability with the correct material positions.
Conclusion
In conclusion, manubriosternal dislocation associated with a chondrosternal joint fracture is rare, and the surgical approach must be based on the surgeon’s experience and procedures that will optimize thoracic cage stability, which must remain the primary objective.
Conflict of interest statement
None to declare.
Funding
No funds were received for the making of this manuscript.

{kind=link}
{kind=link}