





Abstract
Hydatid disease, caused by Echinococcus granulosus, most commonly affects the liver and lungs. Involvement of the head and neck region, particularly the parapharyngeal space, is extremely rare and poses a diagnostic challenge. We report the case of a 13-year-old girl from an endemic area who presented with a painless, rapidly enlarging mass in the right parapharyngeal space, developing over 6 months. Clinical examination revealed a firm, non-tender, transilluminant swelling with intraoral bulging. Computed tomography demonstrated a well-defined cystic lesion in the right parapharyngeal space. The cyst was completely excised via a transcervical approach. Histopathological examination confirmed hydatid cyst, revealing laminated membranes, protoscolices, and daughter cysts. The postoperative course was uneventful, and albendazole was prescribed for two months to prevent recurrence. This case emphasizes considering hydatid disease in the differential diagnosis of cystic neck masses in patients from endemic regions, even in unusual locations.
Introduction
Hydatid cyst is a parasitic zoonosis caused by the larval stage of Echinococcus granulosus, which is endemic in Asia, the Middle East, South America, and Australia [1]. Despite global control efforts, cystic echinococcosis continues to impose a significant health burden, with recent estimates suggesting more than one million affected individuals worldwide, predominantly in pastoral communities where dog–livestock transmission persists [2]. Humans serve as accidental intermediate hosts, with lesions most frequently located in the liver (75%) and lungs (15%), while only ~10% occur in other anatomical sites.
Pediatric cases of cystic echinococcosis are reported less frequently than adult cases, with prevalence increasing steadily with age in community-based surveys, highlighting the importance of vigilance even when children present with cystic lesions in endemic regions [3]. The head and neck region is an uncommon location, and involvement of deep compartments such as the parapharyngeal space is exceedingly rare [4]. Limited arterial dissemination to this region and the non-specific clinical profile contribute to diagnostic delays [5].
Case report
A 13-year-old female, from a rural area in Khyber Pakhtunkhwa, presented with a 6-month history of progressively increasing swelling on the right side of the neck. The swelling was associated with intermittent, mild, non-radiating dull pain that worsened with chewing. She reported no fever, weight loss, constitutional symptoms, or known exposure to livestock or dogs.
On physical examination, a 7 × 4 cm firm, tense, non-tender, non-pulsatile, and immobile swelling was identified extending from the right submandibular region to the parotid area and overlying the mandibular angle. The lesion was transilluminant. Intraoral examination revealed a smooth bulge in the right tonsillar and supratonsillar region, causing medial displacement of the tonsil without mucosal ulceration.
Fine-needle aspiration cytology suggested a benign cystic lesion. Contrast-enhanced computed tomography (CT) of the neck showed a 67 × 38 × 53 mm well-defined cystic mass occupying the right parapharyngeal space, extending from the mandibular condyle in the prestyloid compartment to the mandibular angle (Fig. 1). No daughter cysts, calcifications, or ‘water-lily’ signs were noted.
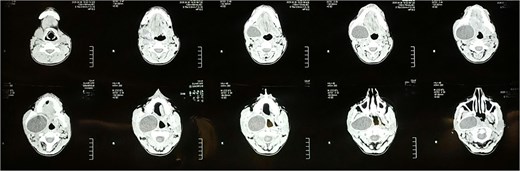
Axial cuts of CT scan showing a well-defined cystic lesion occupying the right parapharyngeal space.
Surgical excision via a transcervical approach was planned. Intraoperatively, a unilocular cyst with smooth borders was visualized deep within the prestyloid parapharyngeal space. The cyst was meticulously dissected from surrounding tissues up to the infratemporal fossa. Care was taken to avoid rupture, and the cyst was removed intact (Fig. 2).
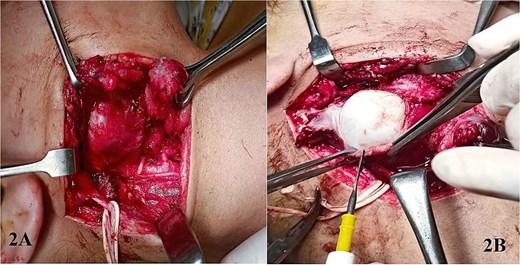
Excision of right parapharyngeal space via transcervical approach with dissection plane reaching to the cystic swelling (A), and then the superficial tissue being dissected meticulously to reveal the optic white walls of the hydatid cyst (B).
Histopathological evaluation confirmed the diagnosis of a hydatid cyst, demonstrating laminated membranes with protoscolices and multiple daughter cysts adherent to the cyst wall.
The postoperative course was uneventful and the 7th post-op day showed healthy wound and return of normal neck contour (Fig. 3). As per standard antihelminthic management, the patient was initiated on albendazole 10–15 mg/kg/day in two divided doses for 2 months, with instructions for monitoring liver function tests during therapy. At her 2-month and 6-month follow-up visits, no evidence of recurrence was noted.

Picture taken of incision site on follow up at 7th postoperative day showing healthy wound and return of normal neck contour.
Discussion
Hydatid disease is an endemic zoonosis with a wide spectrum of presentations, but involvement of the head and neck region remains exceedingly rare. Even within this category, the parapharyngeal space is an exceptional location, with only isolated cases documented in the literature [1, 6]. This rarity contributes to diagnostic difficulty, particularly as lesions in this region typically lack distinctive symptoms and may remain asymptomatic until they reach a considerable size [6].
Radiological imaging is fundamental in evaluating deep neck masses. Although CT and MRI can reveal multiloculated cysts, internal septations, or daughter cysts, features considered suggestive of hydatid disease, such findings are inconsistently present in cervicofacial hydatidosis [5]. In atypical sites such as the parapharyngeal space, hydatid cysts may mimic simple cystic lesions, leading to a broad differential diagnosis that includes branchial cleft cysts, lymphangiomas, salivary gland neoplasms, and neurogenic tumours [5, 7]. In our case, the absence of classical radiological signs contributed to the initial diagnostic ambiguity.
The role of fine needle aspiration cytology (FNAC) remains debated. While several authors report safe use without complications, the potential for cyst rupture, anaphylaxis, and dissemination has led others to discourage its use as a routine diagnostic tool [8, 9]. In this case, FNAC demonstrated only benign cystic features and did not suggest a parasitic origin.
Complete surgical excision without rupture is the treatment of choice for hydatid cysts in the head and neck [10]. The transcervical approach offers direct access to the parapharyngeal space while minimizing neurovascular risk. Avoidance of intraoperative spillage is essential, given reports of anaphylaxis even when cysts remain unruptured [11]. Adjunctive antiparasitic therapy with albendazole is recommended to decrease recurrence risk, particularly when cyst manipulation or incomplete excision is a concern [10].
One limitation of this report is the unavailability of histopathology slide images, as the tissue was processed by an external laboratory owing to resource constraints. Nevertheless, the diagnostic features described are definitive for hydatid disease.
Conclusion
This case report highlights the importance of considering hydatid cyst as a possible differential diagnosis for cystic swellings of the parapharyngeal region. Maintaining a high index of suspicion for cases presenting from rural endemic areas can aid in the better management of this rare entity. It is imperative to perform a meticulous surgical excision to remove the hydatid cyst without spillage of its contents.
Conflict of interest statement
None declared.
Funding
The authors received no funding for this work.

{kind=link}
{kind=link}
{kind=link}