





Abstract
Pylephlebitis of the inferior mesenteric vein is an uncommon complication of sigmoid diverticulitis. A 46-year-old man presented with abdominal pain and features of sepsis. Blood cultures confirmed Bacteroides fragilis bacteraemia, and computed tomography imaging confirmed diverticulitis of the sigmoid colon, complicated by thrombosis of the inferior mesenteric vein. He was managed successfully with empiric antibiotic cover and anticoagulation, before transitioning to ongoing warfarin therapy long term. Treatment for pylephlebitis requires broad-spectrum antibiotic therapy. Anticoagulation is initiated on a case-by-case basis, as no literature consensus exists regarding its utility. Some reports demonstrate a lower rate of thrombotic and septic sequelae in cases where anticoagulation is used for treatment. Surgical treatment remains commonplace in cases of diverticulitis complicated by pylephlebitis. This case describes the presentation and successful management of a case of diverticulitis-associated pylephlebitis, with antibiotic and anticoagulation therapy alone.
Introduction
Diverticulitis, a condition caused by infection and inflammation of diverticular outpouchings of the colon, is a common cause for admission to an acute surgical unit within Australian hospitals [1]. Of those with diverticular disease, 10%–15% will experience at least one episode of diverticulitis [1], with each episode associated with risk of complications. Complications may include perforation, abscess formation, obstruction, fistula, and pylephlebitis [1]. Pylephlebitis is a rare complication (0.2%–0.6%) of intraperitoneal or pelvic infection, particularly in those with an associated bacteraemia [2–5]. Of the portal–mesenteric veins, the inferior mesenteric vein (IMV) is the least commonly affected (2%–6% of cases) [1, 3]. There are no clear clinical features of pylephlebitis; therefore, computed tomography (CT) imaging is essential for prompt diagnosis and management [6]. Features indicating pylephlebitis on CT cross-sectional imaging include subtle contrast enhancement of the venous wall, endoluminal filling defect at the site of thrombus, intraluminal gas, and fat stranding of the surrounding mesentery [1, 3, 6, 7]. It is essential that prompt diagnosis of diverticulitis and associated pylephlebitis is made to prevent increased morbidity and mortality associated with untreated sepsis or thrombus extension and potential ischaemic sequelae [1].
Case report
A 46-year-old man presented with 8 days of left lower quadrant pain with radiation to the left flank. During this time, he experienced associated diarrhoea and subjective fevers. He had a past history of obesity on Ozempic, and type 2 diabetes mellitus on metformin. He had no previous colonoscopy or previous abdominal surgeries. On presentation he was alert and orientated, and his observations were within normal limits aside from a transient tachycardia that resolved after fluid resuscitation. His abdomen was soft, with no features of peritonism, with focal tenderness over the lower abdomen, maximal at the left lower quadrant.
He received intravenous cannulation and initial fluid resuscitation. His blood demonstrated leucocytosis (11.59), C-reactive protein of 213, and a normal coagulation profile. The lactate measured 1.3. CT imaging with portal venous contrast demonstrated sigmoid diverticulitis, complicated by inferior mesenteric vein thrombosis. Features of mesenteric fat stranding were seen surrounding the IMV and left colic branch, with reduced opacification of the vessels in this area (Figs 1 and 2). There was no discrete collection identified. The patient returned a positive blood culture, with growth of Bacteroides fragilis present from the day of admission.

Coronal CT image demonstrating portal venous contrast phase abdomen, with inflammatory fat stranding and wall enhancement of the IMV.
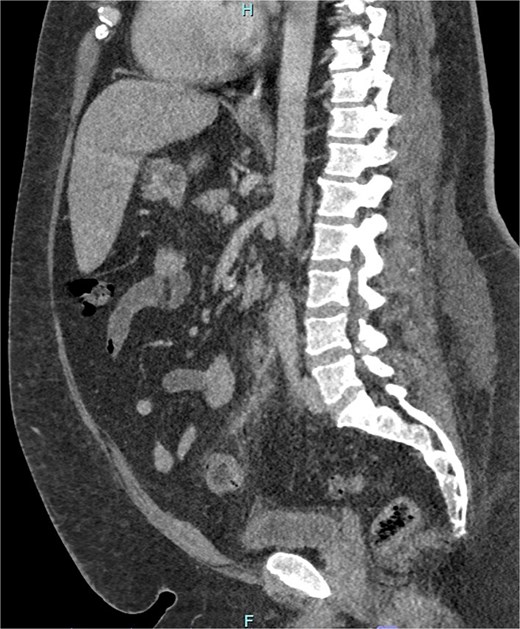
Sagittal CT image demonstrating portal venous contrast phase abdomen, with inflammatory fat stranding and wall enhancement of the IMV and branches.
Management required multispeciality input, including advice from haematology and infectious diseases consultants for treatment of the IMV thrombus and microbiological guidance of antibiotic therapy. With haematological guidance, the patient was commenced on subcutaneous enoxaparin bridging while commencing warfarin, with a plan to achieve an INR of 2–3. Thrombophilia screening was negative. After improvement in the patient’s clinical condition, and associated improvement in inflammatory markers, he was discharged, with a plan for 3 months of anticoagulation and further 5 days of oral antibiotics. He remained well in the community, with no further clinical symptoms of intra-abdominal infection or thrombosis.
Discussion
Infective thrombophlebitis of the IMV, termed ‘pylephlebitis’, is a rare complication of sigmoid diverticulitis [3, 7]. Pylephlebitis refers to septic thrombosis of the portal vein or associated mesenteric branches. Localized inflammation and bacteraemia both contribute to the procoagulopathic milieu thought to drive the development of pylephlebitis. This complication is increasing in incidence, likely secondary to the increased use of CT imaging in the diagnosis of diverticulitis at admission. Imaging findings are required for diagnosis, as symptoms of pylephlebitis are not specific, including abdominal pain, fever, and features of sepsis [1, 8].
Bacteraemia is a risk factor for the development of pylephlebitis, and most commonly includes organisms such as Bacteroides spp., Escherichia coli, Streptococcus spp. Proteus mirabilis, and Klebsiella pneumoniae [3, 7, 9, 10]. Bacteroides fragilis bacteraemia is thought to promote a procoagulopathic environment within the mesenteric circulation secondary to the production of anticardiolipin antibodies and bacterial capsular acceleration of fibrin [2, 10, 11]. Thrombosis in the small perforating veins of the colon results in propagation of thrombosis along the IMV, driven by ongoing sepsis and inflammatory prothrombogenic factors [1, 7]. Sequelae of pylephlebitis can be severe, including septic emboli or abscess formation in downstream organs such as the liver [1]. Thrombotic complications such as extension of thrombosis to portal and hepatic venous circulation [12], or venous ischaemic bowel infarction or splenic infarction, can occur if venous thrombosis is totally occlusive [2, 8].
Management for pylephlebitis requires adequate empiric antibiotic treatment [1, 2, 5, 10, 12]. The role of anticoagulation in pylephlebitis remains controversial, with few large studies reported and thus no literature consensus achieved [3, 4, 6, 7, 10]. Studies reporting outcomes of pylephlebitis managed with anticoagulation do not demonstrate a clear impact on clinical outcomes, particularly in those without coagulation disorders [4, 13]. In a study of 100 cases, 35% received anticoagulation and were found to have improved recanalization and lower mortality than those not anticoagulated [12]. Baril et al., Plemmons et al., and Naymagon et al. reported reduced thrombotic sequelae in those treated with anticoagulation [4, 9, 13]. Anticoagulation is postulated to reduce risk of thrombus extension and assist with thrombus resolution, particularly in cases with extensive thrombus burden and risk of venous ischaemia [4, 8, 10]. Recently reported rates of administration of anticoagulation in these cases is 76.7%–82% [5, 10], with most reported cases involving the use of long-term anticoagulation for 3–6 months [5, 14]. The anticoagulation agent of choice is even less well defined; however, initial treatment with low-molecular-weight heparin and then commencement of an oral anticoagulant on discharge is reported in a few studies [10]. Pinto et al. report successful management of pylephlebitis with heparin bridging to warfarin therapy, which was then switched to rivaroxaban for a duration of 6 months [11].
In many reported cases, pylephlebitis and sepsis is an indication for surgical management of severe diverticulitis [7, 8, 14, 15]. However, this case reports successful conservative management of pylephlebitis with early, appropriate antimicrobial cover and anticoagulation therapy. Fusaro et al. report mortality rates of 8.7%–19% in pylephlebitis, highlighting the importance of further research to determine optimal management of this condition [5, 10].
Conflict of interest statement
The authors have no conflict of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The patient has given informed consent to the publication of images and/or data.

{kind=link}
{kind=link}